 Back
BackBlood: Composition, Functions, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Blood Composition and Functions
Overview of Blood as a Connective Tissue
Blood is a specialized connective tissue composed of a fluid matrix (plasma) and cellular elements (formed elements). It plays a vital role in maintaining homeostasis and supporting physiological processes throughout the body.
Plasma: The liquid component, consisting of water, plasma proteins, and dissolved solutes. Its composition closely resembles interstitial fluid.
Formed Elements: The cellular portion, including erythrocytes (red blood cells), leukocytes (white blood cells), and platelets (thrombocytes).
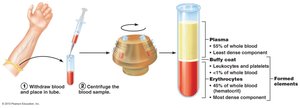
Hematocrit and Blood Separation
Hematocrit is the percentage of blood volume occupied by red blood cells (RBCs). It is a key indicator of oxygen-carrying capacity and varies by sex and physiological state.
Normal Hematocrit Values: 47% ± 5% for males; 42% ± 5% for females.
Leukocytes and Platelets: Together make up about 1% of blood volume (the "buffy coat").
Plasma: Accounts for the remaining blood volume.
Functions of Blood
Blood performs several essential functions:
Transport: Delivers oxygen, nutrients, hormones, and removes metabolic wastes.
Regulation: Maintains pH, electrolyte balance, and body temperature.
Protection: Prevents fluid loss (clotting) and defends against pathogens via white blood cells and antibodies.
Formed Elements of Blood
Classification and Differential Count
The formed elements are classified into erythrocytes, leukocytes, and platelets. Leukocytes are further divided into granulocytes and agranulocytes, each with distinct functions and prevalence in the blood.
Erythrocytes (RBCs): Biconcave, anucleate cells filled with hemoglobin, specialized for gas transport.
Leukocytes (WBCs): Less than 1% of blood volume; capable of diapedesis and chemotaxis. Elevated counts (leukocytosis) indicate infection or inflammation.
Platelets: Cell fragments essential for blood clotting.
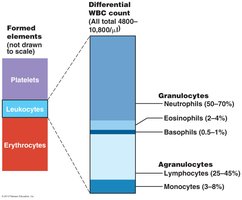
Types of Leukocytes
Neutrophils: Multi-lobed nucleus, fine granules, highly phagocytic; first responders to infection.
Eosinophils: Bi-lobed nucleus, red granules; combat parasitic worms and modulate allergic responses.
Basophils: Rarest WBC, dark granules; release histamine, mediate inflammation, attract other WBCs.
Monocytes: Large cells with U-shaped nucleus; differentiate into macrophages, crucial for phagocytosis.
Lymphocytes: Large, dark nucleus; central to specific immunity (B and T cells).
Blood Typing and Transfusion Compatibility
ABO Blood Groups
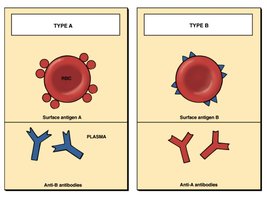
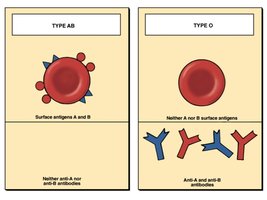
Blood types are determined by the presence or absence of antigens (agglutinogens) A and B on the surface of RBCs. Plasma contains antibodies (agglutinins) against antigens not present on the individual's RBCs.
Type A: Surface antigen A; anti-B antibodies in plasma.
Type B: Surface antigen B; anti-A antibodies in plasma.
Type AB: Both antigens A and B; no anti-A or anti-B antibodies (universal recipient).
Type O: Neither antigen; both anti-A and anti-B antibodies (universal donor).
ABO Compatibility Table
The following table summarizes the compatibility of ABO blood groups, including antigens, antibodies, and transfusion possibilities.
Blood Group | RBC Antigens | Plasma Antibodies | Blood That Can Be Received | Frequency in U.S. Population (%) |
|---|---|---|---|---|
AB | A, B | None | A, B, AB, O | White: 4 Black: 4 Asian: 7 Native American: <1 |
B | B | Anti-A | B, O | White: 10 Black: 19 Asian: 27 Native American: 13 |
A | A | Anti-B | A, O | White: 40 Black: 27 Asian: 28 Native American: 16 |
O | None | Anti-A, Anti-B | O | White: 45 Black: 49 Asian: 39 Native American: 79 |

Blood Typing Reactions
Blood typing is performed by mixing blood with anti-A and anti-B sera. Agglutination indicates the presence of the corresponding antigen.

Rh Blood Groups and Clinical Implications
Rh Factor
The Rh blood group is determined by the presence or absence of the D antigen (Rh factor) on RBCs. Rh+ individuals have the D antigen; Rh– individuals do not. Anti-Rh antibodies are only produced after exposure to Rh+ blood.
Rh+: D antigen present.
Rh–: D antigen absent; can develop anti-Rh antibodies after exposure.
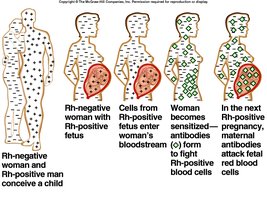
Hemolytic Disease of the Newborn (Erythroblastosis Fetalis)
This condition occurs when an Rh– mother is sensitized by exposure to Rh+ fetal blood, leading to the production of anti-Rh antibodies. In subsequent pregnancies, these antibodies can cross the placenta and destroy fetal RBCs if the fetus is Rh+.
Prevention: Administration of RhoGAM to Rh– mothers prevents sensitization.
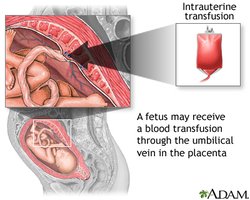
Treatment: Intrauterine and exchange transfusions may be required for affected infants.
Laboratory Technique: Wright’s Stain Procedure
Steps for Blood Smear Preparation and Staining
Wright’s stain is used to differentiate blood cell types on a microscope slide. The procedure involves:
Prepare a blood film and air dry.
Apply Wright’s stain, wait, then add water and mix.
Rinse, dry, and examine microscopically.
Safety Note: Wright’s stain is hazardous; avoid skin contact.
