 Back
BackBlood: Structure, Function, and Clinical Aspects (Chapter 17 Study Notes)
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Blood: Structure, Function, and Clinical Aspects
Overview of Blood Functions
Blood is a specialized connective tissue that serves as the body's internal transport system. It performs three primary functions: transport, regulation, and protection.
Transport: Delivers oxygen and nutrients to cells, removes metabolic waste to lungs and kidneys, and transports hormones from endocrine organs to target organs.
Regulation: Maintains body temperature, pH balance (using buffers and bicarbonate ions), and fluid volume.
Protection: Prevents blood loss (clotting) and infection (immune cells and proteins).
Composition of Blood
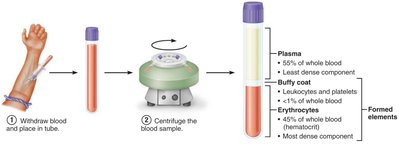
Blood consists of plasma (liquid matrix) and formed elements (cells and cell fragments). When centrifuged, blood separates into three layers:
Plasma: ~55% of blood; mostly water with dissolved solutes (proteins, nutrients, gases, hormones, wastes, ions).
Buffy coat: <1% of blood; contains leukocytes (WBCs) and platelets.
Erythrocytes: ~45% of blood (hematocrit); red blood cells (RBCs).
Blood Plasma
Plasma is a straw-colored, sticky fluid that is about 90% water. It contains over 100 dissolved solutes, including:
Electrolytes: Sodium, potassium, calcium, chloride, bicarbonate, etc.
Plasma proteins: Albumin (60%, maintains osmotic pressure), globulins (transport and immune functions), fibrinogen (clotting).
Nutrients, gases, hormones, wastes, and nonprotein nitrogenous substances.
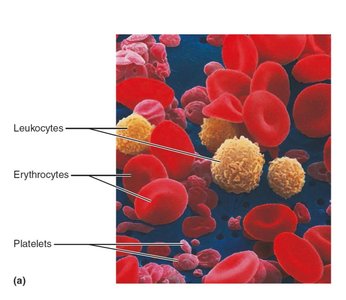
Formed Elements of Blood
The formed elements include erythrocytes, leukocytes, and platelets. Most are short-lived and arise from stem cells in red bone marrow.
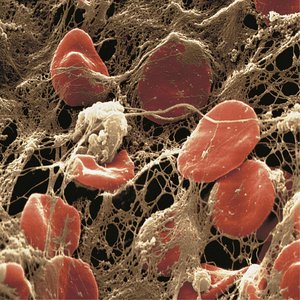
Erythrocytes (RBCs): Anucleate, biconcave discs specialized for gas transport.
Leukocytes (WBCs): Complete cells involved in immune defense.
Platelets: Cell fragments essential for blood clotting.
Erythrocytes (Red Blood Cells)
Structure and Function
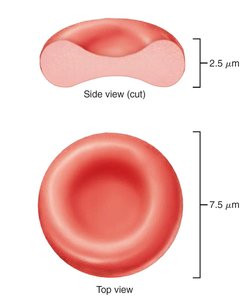
Erythrocytes are small, biconcave, anucleate cells filled with hemoglobin (Hb) for oxygen and carbon dioxide transport. Their shape increases surface area for gas exchange and allows flexibility in capillaries.
Diameter: ~7.5 μm; Thickness: ~2.5 μm at thickest point.
No mitochondria: ATP is produced anaerobically, so RBCs do not consume the oxygen they transport.
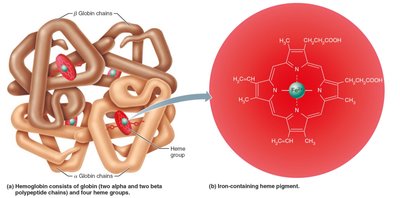
Hemoglobin Structure and Function
Hemoglobin is a protein composed of four polypeptide chains (two alpha, two beta), each with a heme group containing an iron ion. Each iron binds one O2 molecule, so each Hb can carry four O2 molecules.
Oxygen transport: O2 binds to iron in heme (oxyhemoglobin in lungs, deoxyhemoglobin in tissues).
Carbon dioxide transport: 20% of CO2 binds to globin (carbaminohemoglobin).
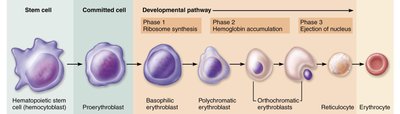
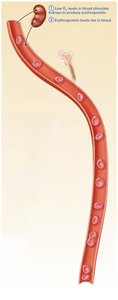
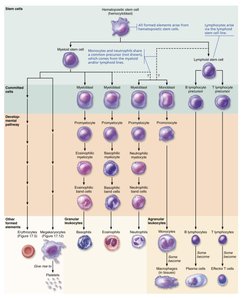
Erythropoiesis: Formation of Red Blood Cells
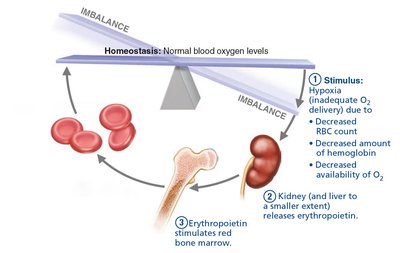
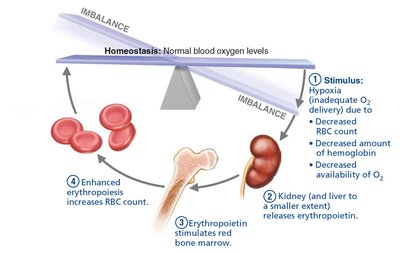
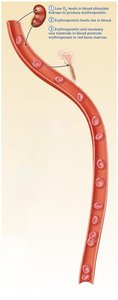
Erythropoiesis occurs in red bone marrow and is regulated by erythropoietin (EPO), a hormone produced by the kidneys in response to hypoxia (low O2 levels).
Stages: Hematopoietic stem cell → Myeloid stem cell → Proerythroblast → Erythroblast stages (basophilic, polychromatic, orthochromatic) → Reticulocyte → Erythrocyte.
Regulation: EPO stimulates RBC production; dietary requirements include iron, vitamin B12, folic acid, amino acids, and lipids.
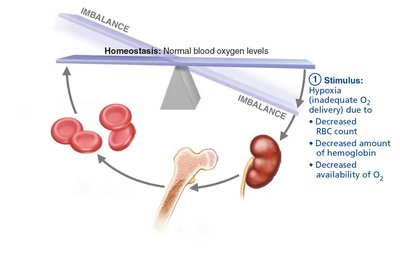
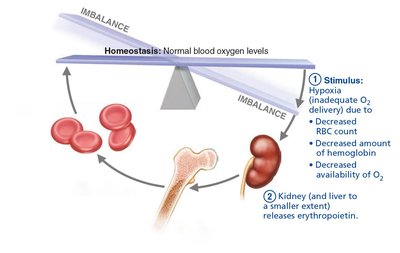
Regulation of Erythropoiesis
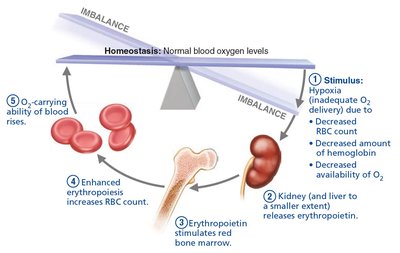
The number of circulating RBCs is maintained by a balance between production and destruction. EPO release is triggered by hypoxia, and its effects are enhanced by testosterone.
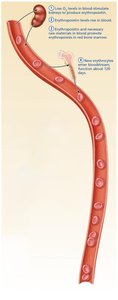
Negative feedback loop: Low O2 → EPO release → Increased RBC production → Restored O2 levels → Inhibition of EPO.
Life Cycle and Fate of Erythrocytes
RBCs live about 100–120 days. Old RBCs are removed by macrophages in the spleen, and their components are recycled or excreted.
Iron: Stored and reused.
Heme: Degraded to bilirubin, excreted in bile.
Globin: Broken down to amino acids.


Erythrocyte Disorders
Anemia: Reduced O2-carrying capacity due to blood loss, decreased RBC production, or increased RBC destruction.
Sickle-cell anemia: Genetic disorder causing abnormal hemoglobin and sickle-shaped RBCs.
Polycythemia: Excess RBCs, increasing blood viscosity.

Leukocytes (White Blood Cells)
Structure and Function
Leukocytes are complete cells that defend the body against pathogens. They can leave the bloodstream (diapedesis) and move toward infection sites (chemotaxis).
Normal count: 4,800–10,800/μL
Leukocytosis: Elevated WBC count, often due to infection.
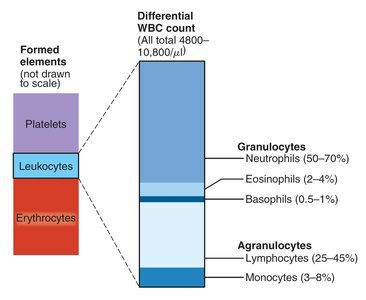
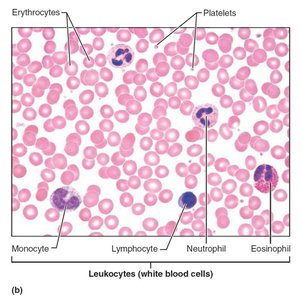
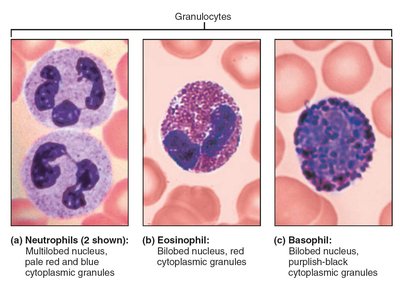
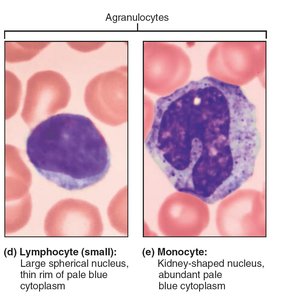
Types of Leukocytes
Granulocytes: Neutrophils (phagocytize bacteria), eosinophils (combat parasites, modulate allergies), basophils (release histamine).
Agranulocytes: Lymphocytes (T cells and B cells for immunity), monocytes (differentiate into macrophages).
Leukopoiesis: Formation of White Blood Cells
Leukopoiesis is stimulated by interleukins and colony-stimulating factors. Hematopoietic stem cells differentiate into myeloid or lymphoid lines, producing all WBC types.
Leukocyte Disorders
Leukopenia: Abnormally low WBC count, often drug-induced.
Leukemia: Cancerous overproduction of abnormal WBCs.
Infectious mononucleosis: Viral disease causing excess atypical lymphocytes.
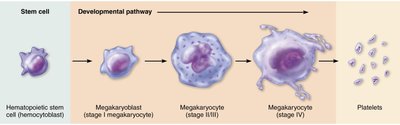
Platelets and Hemostasis
Platelets: Structure and Function
Platelets are fragments of megakaryocytes essential for blood clotting. They form a temporary plug at sites of vessel injury and release chemicals that promote clotting.
Summary Table: Formed Elements of Blood
Cell Type | Description | Count (per μL) | Development Time | Life Span | Function |
|---|---|---|---|---|---|
Erythrocytes | Biconcave, anucleate | 4–6 million | ~15 days | 100–120 days | Transport O2 and CO2 |
Neutrophils | Multilobed nucleus, granules | 3,000–7,000 | ~14 days | 6 hrs–few days | Phagocytize bacteria |
Eosinophils | Bilobed nucleus, red granules | 100–400 | ~14 days | ~5 days | Kill parasites, allergy/asthma |
Basophils | Bilobed nucleus, purple granules | 20–50 | 1–7 days | hrs–few days | Release histamine |
Lymphocytes | Spherical nucleus | 1,500–3,000 | days–weeks | hrs–years | Immunity |
Monocytes | U/kidney-shaped nucleus | 100–700 | 2–3 days | months | Phagocytosis |
Platelets | Fragments, granules | 150,000–400,000 | 4–5 days | 5–10 days | Clotting |
Hemostasis: Prevention of Blood Loss
Hemostasis is a rapid, localized process to stop bleeding, involving three steps:
Vascular spasm: Vasoconstriction of damaged vessel.
Platelet plug formation: Platelets adhere to exposed collagen and aggregate.
Coagulation: Fibrin mesh reinforces the plug, forming a stable clot.



Coagulation Pathways
Coagulation involves a cascade of clotting factors, leading to the conversion of fibrinogen to fibrin. There are two pathways:
Intrinsic pathway: Triggered by factors within blood.
Extrinsic pathway: Triggered by tissue factor outside blood.
Both pathways converge to activate prothrombin, which is converted to thrombin, then fibrinogen to fibrin.



Clot Retraction and Fibrinolysis
After vessel repair, the clot is stabilized (retraction) and then dissolved (fibrinolysis) by plasmin, which digests fibrin.
Disorders of Hemostasis
Thromboembolic disorders: Unwanted clot formation (thrombus, embolus).
Bleeding disorders: Thrombocytopenia (low platelets), impaired liver function, hemophilia (clotting factor deficiency).
Disseminated intravascular coagulation (DIC): Both clotting and bleeding occur.

Blood Transfusion and Blood Typing
Blood Groups and Transfusion
Blood transfusions require compatibility of ABO and Rh blood groups to prevent transfusion reactions. Antigens (agglutinogens) on RBCs determine blood type; antibodies (agglutinins) in plasma react with foreign antigens.
ABO system: Type A (A antigen), B (B antigen), AB (A and B antigens, universal recipient), O (no antigens, universal donor).
Rh system: Rh+ (D antigen present), Rh− (D antigen absent).
Clinical Applications and Blood Tests
Blood tests provide diagnostic information (e.g., hematocrit, CBC, differential WBC count, blood chemistry). Blood diseases can indicate systemic disorders.
Developmental Aspects of Blood
Blood cell formation shifts from the yolk sac, liver, and spleen in the fetus to red bone marrow by the seventh month. Fetal hemoglobin (HbF) has a higher affinity for oxygen than adult hemoglobin (HbA).
