Back
BackBones and Skeletal Tissues: Structure, Function, and Development
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Bones and Skeletal Tissues
Introduction
The human skeleton is a dynamic organ system essential for support, movement, protection, and metabolic functions. Understanding bone anatomy and physiology is crucial for diagnosing and treating skeletal disorders.
Skeletal Cartilages
Basic Structure, Types, and Locations
Skeletal cartilage is made of resilient, molded cartilage tissue, primarily water, with no blood vessels or nerves.
Perichondrium is a dense connective tissue layer surrounding cartilage, providing nutrients and resisting expansion.
Cartilage cells, chondrocytes, are found in lacunae within a jelly-like matrix.
Types of Cartilage
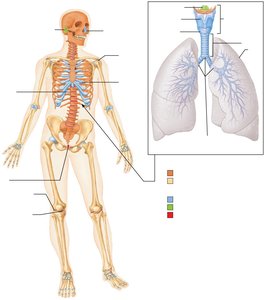
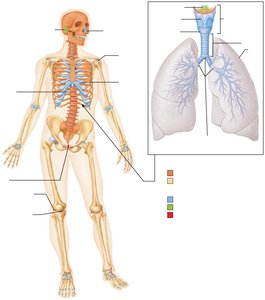
Hyaline cartilage: Most abundant; provides support, flexibility, and resilience. Locations: articular surfaces, costal cartilage, respiratory structures, nasal cartilage.
Elastic cartilage: Contains elastic fibers; found in the external ear and epiglottis.
Fibrocartilage: Thick collagen fibers; high tensile strength. Locations: menisci of knee, intervertebral discs.
Growth of Cartilage
Appositional growth: New matrix is secreted on the surface by cells in the perichondrium.
Interstitial growth: Chondrocytes divide and secrete new matrix from within the cartilage.
Calcification: Occurs during normal bone growth and aging; calcified cartilage is not bone.
Functions of Bones
Major Functions
Support: Framework for the body and soft organs.
Protection: Shields brain, spinal cord, and vital organs.
Movement: Acts as levers for muscle action.
Mineral and growth factor storage: Reservoir for calcium, phosphorus, and growth factors.
Blood cell formation: Hematopoiesis in red marrow cavities.
Triglyceride storage: Fat storage in bone cavities.
Hormone production: Osteocalcin regulates insulin, glucose, and metabolism.
Classification of Bones
By Location
Axial skeleton: Skull, vertebral column, rib cage.
Appendicular skeleton: Limbs and girdles.
By Shape
Long bones: Longer than wide (e.g., limb bones).
Short bones: Cube-shaped (wrist, ankle); sesamoid bones (e.g., patella).
Flat bones: Thin, flat, slightly curved (sternum, scapulae, ribs, skull).
Irregular bones: Complicated shapes (vertebrae, hip bones).
Bone Structure
Gross Anatomy
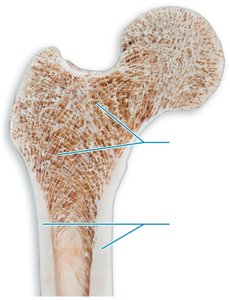
Compact bone: Dense outer layer; smooth and solid.
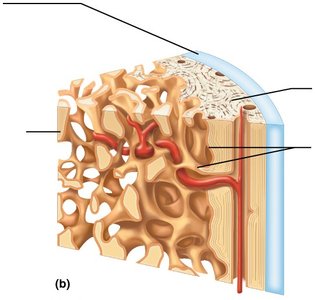
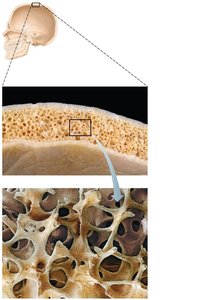
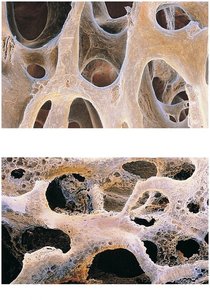
Spongy bone: Honeycomb of trabeculae filled with marrow.
Structure of Short, Irregular, and Flat Bones
Thin plates of spongy bone (diploë) covered by compact bone.
Periosteum covers outside; endosteum covers inside.
No defined marrow cavity; marrow is scattered throughout spongy bone.

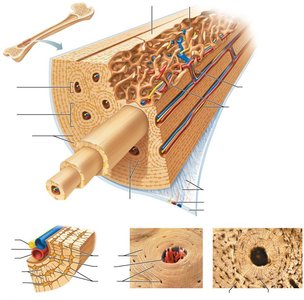
Structure of a Typical Long Bone
Diaphysis: Shaft; compact bone surrounds medullary cavity (yellow marrow in adults).
Epiphyses: Bone ends; compact bone externally, spongy bone internally; articular cartilage covers joint surfaces.
Epiphyseal line: Remnant of growth plate between diaphysis and epiphysis.

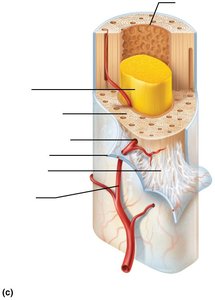
Membranes
Periosteum: Double-layered membrane; outer fibrous layer (dense irregular CT), inner osteogenic layer (bone-forming cells).
Endosteum: Delicate membrane covering internal bone surfaces, trabeculae, and canals.
Hematopoietic Tissue
Red marrow: Found in spongy bone and diploë of flat bones; active in hematopoiesis.
Yellow marrow: Can convert to red marrow if needed (e.g., anemia).
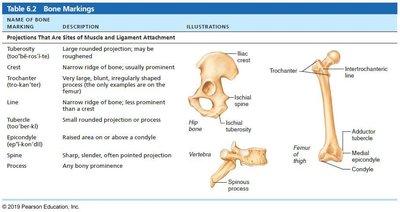
Bone Markings
Bone markings serve as sites for muscle, ligament, and tendon attachment, joint formation, and passageways for blood vessels and nerves.
Name of Bone Marking | Description | Illustration |
|---|---|---|
Tuberosity | Large rounded projection; may be roughened | Femur |
Crest | Narrow ridge of bone; usually prominent | Ilium |
Trochanter | Very large, blunt, irregularly shaped process | Femur |
Line | Narrow ridge of bone; less prominent than a crest | Femur |
Tubercle | Small rounded projection or process | Humerus |
Epicondyle | Raised area on or above a condyle | Femur |
Spine | Sharp, slender, often pointed projection | Vertebra |
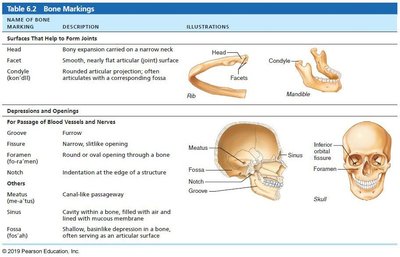
Name of Bone Marking | Description | Illustration |
|---|---|---|
Head | Bony expansion carried on a narrow neck | Femur |
Facet | Smooth, nearly flat articular surface | Rib |
Condyle | Rounded articular projection | Mandible |
Foramen | Round or oval opening through a bone | Skull |
Fossa | Shallow, basinlike depression in a bone | Skull |
Microscopic Anatomy of Bone
Bone Cells
Osteogenic cells: Stem cells in periosteum and endosteum; differentiate into osteoblasts or bone-lining cells.
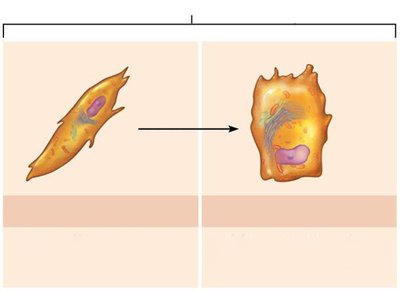
Osteoblasts: Bone-forming cells; secrete osteoid (collagen and calcium-binding proteins).
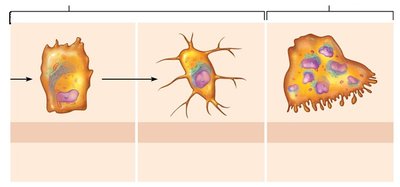
Osteocytes: Mature bone cells in lacunae; maintain matrix and act as stress sensors.
Bone-lining cells: Flat cells on bone surfaces; help maintain matrix.
Osteoclasts: Multinucleate cells; resorb bone matrix.

Compact Bone Structure
Osteon (Haversian system): Structural unit; concentric lamellae around a central canal.
Canals and canaliculi: Central (Haversian) canal, perforating (Volkmann's) canals, lacunae, and canaliculi for nutrient/waste exchange.
Lamellae: Interstitial (fill gaps) and circumferential (encircle diaphysis).
Spongy Bone Structure
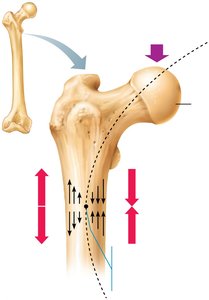
Trabeculae align along lines of stress; contain irregular lamellae and osteocytes connected by canaliculi.
Capillaries in endosteum supply nutrients.
Chemical Composition of Bone
Organic components: Cells and osteoid (collagen, ground substance); provide tensile strength and flexibility.
Inorganic components: Hydroxyapatites (calcium phosphate crystals); provide hardness and resistance to compression.
Bone Development (Ossification)
Ossification Types
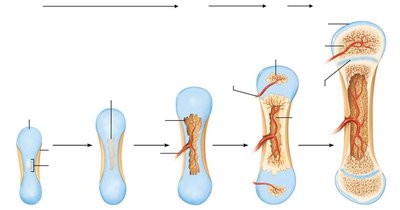
Endochondral ossification: Bone replaces hyaline cartilage; forms most of the skeleton.
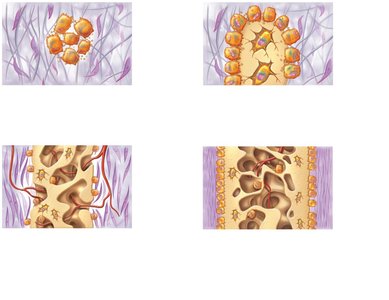
Intramembranous ossification: Bone develops from fibrous membrane; forms flat bones of skull and clavicle.
Postnatal Bone Growth
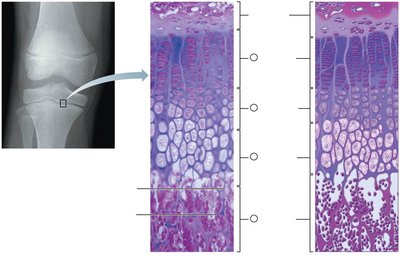
Interstitial growth: Lengthening at the epiphyseal plate (five zones: resting, proliferation, hypertrophic, calcification, ossification).
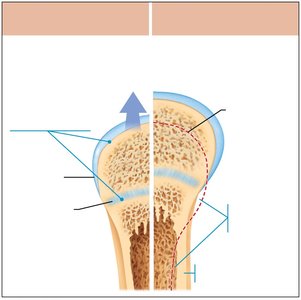
Appositional growth: Increase in bone thickness.
Hormonal Regulation
Growth hormone: Stimulates epiphyseal plate activity.
Thyroid hormone: Modulates growth hormone effects.
Sex hormones: Promote growth spurts and epiphyseal plate closure.
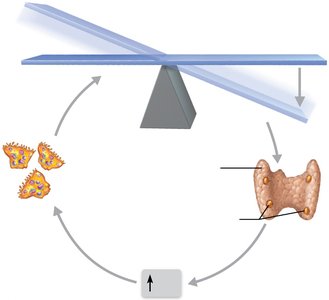
Bone Remodeling
Continuous process of bone deposit (by osteoblasts) and resorption (by osteoclasts).
Regulated by hormonal controls (parathyroid hormone, calcitonin) and mechanical stress (Wolff's law).
Bone Repair
Fracture Classification
By position: nondisplaced vs. displaced
By completeness: complete vs. incomplete
By skin penetration: open (compound) vs. closed (simple)
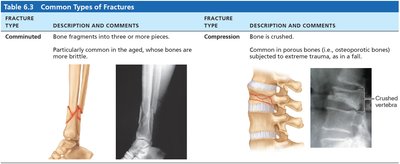
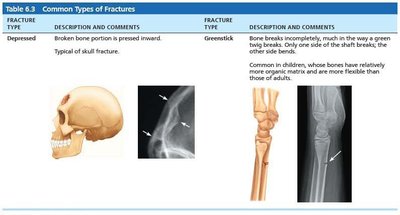
Fracture Type | Description and Comments |
|---|---|
Comminuted | Bone fragments into three or more pieces; common in aged |
Compression | Bone is crushed; common in porous bones |
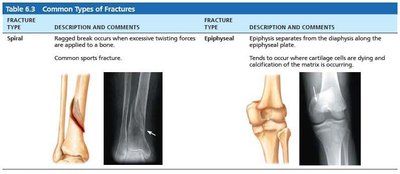
Spiral | Ragged break from twisting forces; common sports fracture |
Epiphyseal | Epiphysis separates from diaphysis along plate |
Depressed | Broken bone pressed inward; typical of skull fracture |
Greenstick | Bone breaks incompletely; common in children |
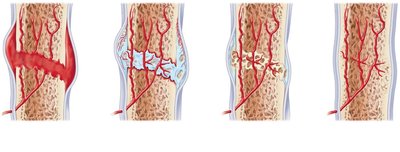
Fracture Repair Stages
Hematoma formation
Fibrocartilaginous callus formation
Bony callus formation
Bone remodeling
Bone Disorders
Osteomalacia and Rickets
Poor mineralization; soft, weak bones; pain on weight-bearing.
Rickets in children: bowed legs, bone deformities; caused by vitamin D or calcium deficiency.
Osteoporosis
Bone resorption exceeds deposit; bone mass declines; common in spine and femur.
Risk factors: age, postmenopausal women, low exercise, poor diet, smoking, genetics, hormone disorders.
Treatments: calcium, vitamin D, exercise, hormone therapy, bisphosphonates, denosumab.
Prevention: adequate calcium, reduced alcohol, weight-bearing exercise.
Paget’s Disease
Excessive, disorganized bone remodeling; high spongy to compact bone ratio; reduced mineralization.
Common in spine, pelvis, femur, skull; treated with calcitonin and bisphosphonates.

Developmental Aspects of Bone
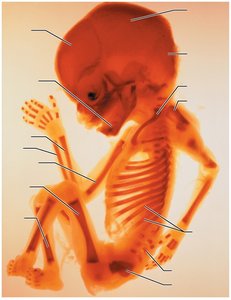
Embryonic skeleton ossifies predictably; fetal age can be determined by X-ray.
Most long bones ossify by 8 weeks; primary centers by week 12.
At birth, most long bones are ossified except at epiphyses; complete ossification by ~age 25.
Bone formation exceeds resorption in children; balanced in young adults; resorption exceeds formation in older adults.