 Back
BackCardiac Muscle, Conduction System, Electrocardiography, and Cardiac Cycle
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Module 4 part 2
Cardiac Muscle Structure and Function
Characteristics of Cardiac Muscle Cells
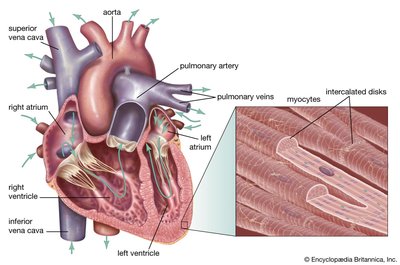
Cardiac muscle cells, or myocytes, are specialized for continuous rhythmic contraction and are structurally distinct from skeletal muscle fibers.
Striated Appearance: Cardiac muscle is striated due to the arrangement of actin and myosin filaments, similar to skeletal muscle.
Cell Shape: Cardiac cells are short, fat, branched, and interconnected, unlike the long, cylindrical, multinucleated skeletal muscle fibers.
Nuclei: Each cardiac cell contains one or two centrally located nuclei.
Endomysium: The intercellular spaces are filled with a loose connective tissue matrix (endomysium) containing numerous capillaries, which connects to the dense fibrous skeleton of the heart.
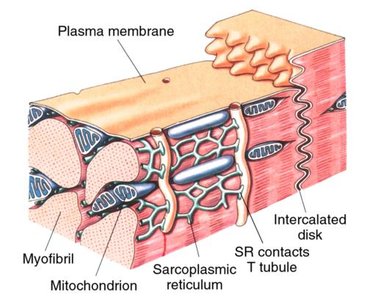
Intercalated Discs: Cardiac cells interconnect at junctions called intercalated discs, which contain anchoring desmosomes and gap junctions.
Desmosomes: Prevent separation of adjacent cells during contraction.
Gap Junctions: Allow ions to pass from cell to cell, enabling direct transmission of the depolarizing impulse across the heart, so the myocardium acts as a functional syncytium.
Automaticity and Rhythmicity
Cardiac muscle cells possess unique properties that allow the heart to function independently and rhythmically.
Automaticity: Some cardiac cells are self-excitable and can initiate their own depolarization due to leaky plasma membranes, allowing sodium and calcium ions to enter easily.
Rhythmicity: Cardiac cells contract in a definite rhythm, typically set by the pacemaker (SA node).Sinoatrial Node
Resting Membrane Potential: Cardiac contractile cells remain at rest until excited by the pacemaker, with a resting membrane potential of -90mV.
Refractory Period: The refractory period is longer in cardiac muscle than in skeletal muscle, preventing tetanic contractions and ensuring effective pumping.
Mechanism and Events of Cardiac Muscle Contraction
The contraction of cardiac muscle follows a sequence similar to skeletal muscle but with key differences.
Action Potential Initiation: Influx of sodium ions initiates the action potential by opening voltage-regulated sodium channels.
Calcium Entry: Depolarization down T-tubules causes calcium entry into the sarcoplasm. Calcium is required for crossbridge activation and couples depolarization to myofilament sliding (excitation-contraction coupling).
Calcium Sources: Cardiac muscle relies on both extracellular calcium entry and release from the sarcoplasmic reticulum.
Repolarization: Calcium ions are pumped back into the sarcoplasmic reticulum and extracellular space during repolarization.
Energy Requirements
Cardiac muscle is highly dependent on aerobic metabolism.
Mitochondria: Cardiac muscle has more mitochondria than skeletal muscle, reflecting its reliance on oxygen.
Fuel Preference: Cardiac muscle uses fatty acids more effectively for ATP production, while skeletal muscle prefers glucose during activity.
Intrinsic Cardiac Conduction System
Overview of the Conduction System
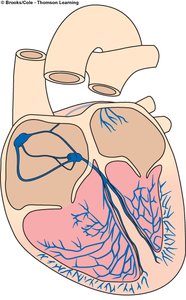
The heart's ability to depolarize and contract is intrinsic, relying on specialized cells and gap junctions.
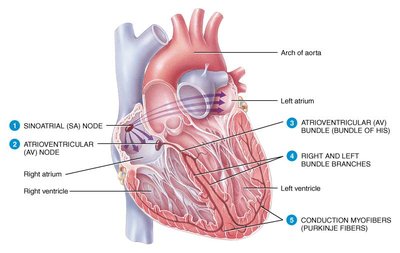
Components: The conduction system includes the SA node, AV node, AV bundle (bundle of His), right and left bundle branches, and Purkinje fibers.
Function: These components ensure orderly, sequential depolarization and contraction from atria to ventricles.
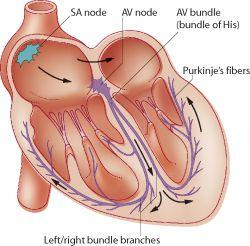
Key Components of the Conduction System
Sinoatrial (SA) Node: Located in the right atrial wall, the SA node is the pacemaker, spontaneously depolarizing 70-80 times per minute and setting the sinus rhythm.
Atrioventricular (AV) Node: Located in the interatrial septum, the AV node delays the impulse, allowing atrial contracf vgjnhkm,l./tion before ventricular excitation.
AV Bundle (Bundle of His): Transmits the impulse from the AV node to the bundle branches.
Bundle Branches: Carry the impulse through the interventricular septum.
Purkinje Fibers: Penetrate the ventricular myocardium, stimulating contraction of the papillary muscles and ventricles.
Electrocardiography (ECG)
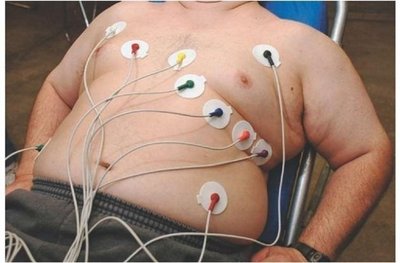
Principles of Electrocardiography
Electrocardiography records the electrical activity of the heart using electrodes placed on the body surface.
ECG: A recording of the heart's electrical events, useful for diagnosing arrhythmias and conduction abnormalities.
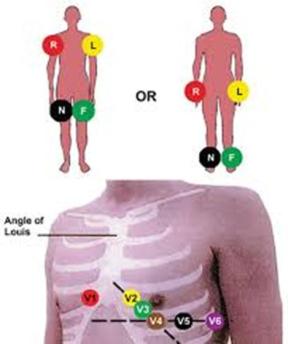
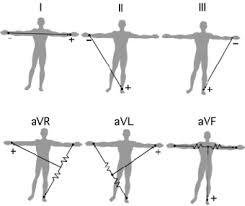
Leads: A 12-lead ECG provides 12 views of the heart using 10 electrodes.
Lead II: Commonly used for monitoring, views the inferior aspect of the left myocardium.
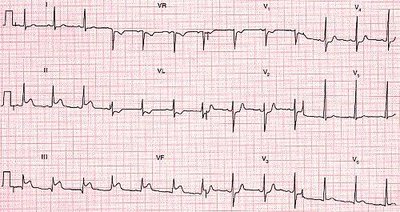
ECG Waves and Intervals
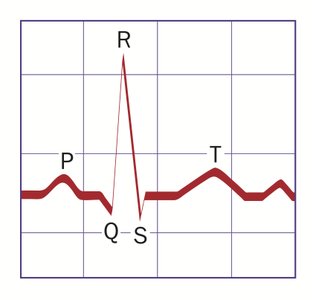
A typical ECG consists of three main waves and several intervals.
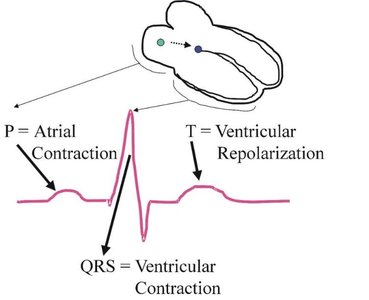
P Wave: Represents atrial depolarization (contraction), lasts about 0.08 seconds.
QRS Complex: Represents ventricular depolarization (contraction), lasts about 0.08 seconds, and masks atrial repolarization.
T Wave: Represents ventricular repolarization (relaxation), lasts about 0.16 seconds.
P-R Interval: Time from beginning of atrial excitation to beginning of ventricular excitation (~0.16 seconds).
Q-T Interval: Time from beginning of ventricular depolarization through repolarization (~0.36 seconds).
ECG Analysis and Arrhythmias
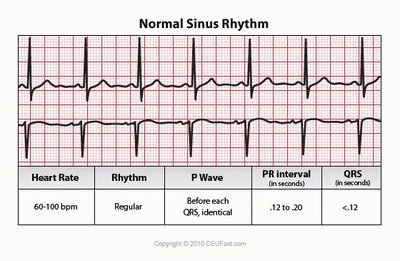
Normal Sinus Rhythm (NSR): P wave, QRS complex, and T wave are present and consistent.
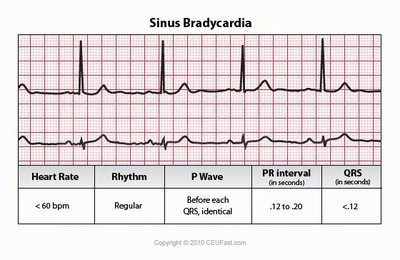
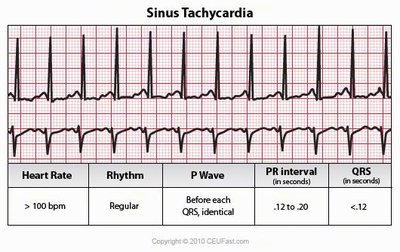
Arrhythmias: Abnormal patterns of cardiac activity, including bradycardia, tachycardia, heart blocks, and fibrillation.
Clinical Significance: Changes in ECG pattern or timing may indicate myocardial infarct or conduction system problems.
ECG Patterns in Heart Blocks
Partial AV Block: Every other P wave fails to evoke QRST.
Complete AV Block: P waves and QRST occur independently.



Cardiac Cycle
Overview of the Cardiac Cycle
The cardiac cycle is the sequence of events in one heartbeat, including contraction (systole) and relaxation (diastole) of the atria and ventricles.
Systole: Contraction phase, blood is ejected from the chambers.
Diastole: Relaxation phase, chambers refill with blood.
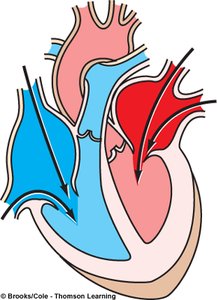
Pressure Changes: Blood flows along a pressure gradient, causing opening and closing of heart valves.
Phases of the Cardiac Cycle
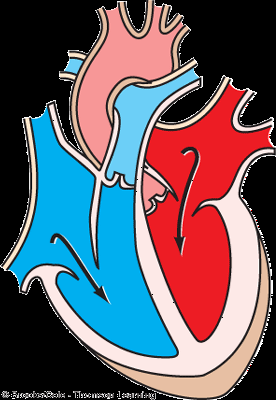
Ventricular Filling (mid-to-late diastole): Blood flows passively into ventricles, AV valves open, semilunar valves closed. About 70% of ventricular filling occurs during this phase.
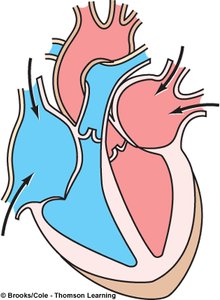
Atrial Systole: Atria contract, propelling remaining blood into ventricles.
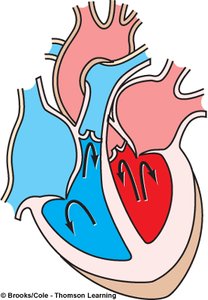
Isovolumetric Ventricular Contraction: Ventricles contract, AV valves close, semilunar valves remain closed, pressure rises.
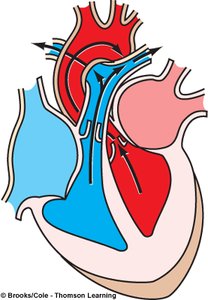
Ventricular Ejection: Semilunar valves open, blood is expelled into aorta and pulmonary trunk.
Isovolumetric Relaxation (early diastole): Ventricles relax, semilunar valves close, AV valves remain closed, atria fill with blood.
Timing of the Cardiac Cycle
Average Heart Rate: 75 beats per minute.
Cycle Length: About 0.8 seconds per cycle.
Atrial Systole: 0.1 second.
Ventricular Systole: 0.3 second.
Quiescent Period (Total Relaxation): 0.4 second.
Heart Sounds
The cardiac cycle produces characteristic heart sounds.
LUBB: First sound, caused by closure of AV valves during ventricular systole.
DUP: Second sound, caused by closure of semilunar valves during ventricular diastole.
Heart Murmurs: Extra sounds caused by improper closure of valves.
Summary Table: Cardiac Cycle Phases
Phase | Valves Open | Valves Closed | Event |
|---|---|---|---|
Ventricular Filling | AV (mitral, tricuspid) | Semilunar (aortic, pulmonic) | Passive blood flow into ventricles |
Atrial Systole | AV (mitral, tricuspid) | Semilunar (aortic, pulmonic) | Atria contract, active filling of ventricles |
Isovolumetric Contraction | None | All | Ventricles contract, pressure rises |
Ventricular Ejection | Semilunar (aortic, pulmonic) | AV (mitral, tricuspid) | Blood ejected from ventricles |
Isovolumetric Relaxation | None | All | Ventricles relax, atria fill |
Key Terms and Definitions
Syncytium: A group of cells that function as a single unit due to electrical coupling.
Automaticity: The ability of cardiac cells to initiate their own depolarization.
Arrhythmia: Abnormal heart rhythm.
Systole: Contraction phase of the heart.
Diastole: Relaxation phase of the heart.
ECG: Electrocardiogram, a recording of the heart's electrical activity.
Relevant Equations
Cardiac Output:
Stroke Volume:
Example
ECG Interpretation: A normal ECG shows regular P waves, QRS complexes, and T waves, indicating normal sinus rhythm. Abnormalities such as missing P waves or irregular QRS complexes may indicate arrhythmias or heart blocks.
Additional info: Academic context was added to clarify the mechanisms of cardiac muscle contraction, conduction system, ECG interpretation, and cardiac cycle phases.
