 Back
BackCardiac Output and Its Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Cardiac Output and Regulation
Introduction to Cardiac Output
Cardiac output (CO) is the amount of blood pumped by each ventricle (pulmonary + systemic circuit) in one minute. It is a critical parameter for maintaining adequate tissue perfusion and is determined by two main factors: heart rate (HR) and stroke volume (SV).
Heart Rate (HR): The number of cardiac cycles (beats) per minute, typically 60–80 bpm in adults.
Stroke Volume (SV): The amount of blood ejected by a ventricle with each heartbeat, usually about 70 mL at rest. (CONSTANT)
Can be determined easily by subtracting the amount of blood in the ventricle at the end of a contraction (ESV) & the amount of blood in the ventricle after it has filled during diastole (EDV)
Average Heart: 120ml (ESV) - 50 ml (EDV) =70 mL (Stroke Volume)
Cardiac Output (CO): Calculated as .
Example Calculation: , or approximately 5 liters per minute.
The right ventricle pumps about 5ml into the pulmonary circuit and the left ventricle pumps the same amount into the systemic circuit in 1 minute.
Determinants of Stroke Volume
Stroke volume is difficult to measure directly often measured by the ejection fraction is the percentage of blood (out of the total amount) that is ejected with each ventricular systole, and is equal to the stroke volume divided by the EDV.
Normal Ejection fraction is 50-65% and the value should be equal for each ventricle.
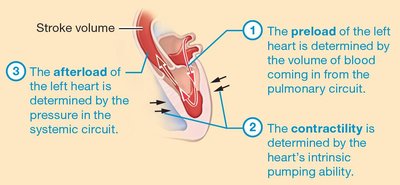
Stroke Volume is influenced by three primary factors: preload, contractility, and afterload. These factors determine how much blood the heart pumps with each beat.
Preload: The degree of stretch of cardiac muscle cells before contraction, largely determined by end-diastolic volume (EDV).
Contractility: The intrinsic ability of cardiac muscle to contract at a given fiber length, influenced by inotropic agents. (Ability to generate Tension)
Afterload: The resistance the ventricles must overcome to eject blood, primarily determined by arterial blood pressure.
Preload involved EDV while Contractility and Afterload affect the ESV.
Preload
Preload is the initial stretching of the cardiac muscle cell/ sarcomere prior to contraction, related to the volume of blood returning to the heart (venous return) and the duration of ventricular diastole. (amount of blood that has drained into the ventricle by the end of the filling phase)
Increased preload leads to increased EDV, stretching the ventricular walls and resulting in a more forceful contraction (Frank-Starling law).
Frank-Starling law: the more ventricular muscle cells are stretched , the more forcefully they contract
Factors increasing preload: longer diastole, increased venous return.
This relationship is particularly important during exercise, when cardiac output must increase to meet the body’s needs.
Contractility
Contractility refers to the strength of contraction at a given preload, influenced by the autonomic nervous system and circulating hormones.
Ability to generate tension, in the absence of any external influences such as stretch
Can be estimated clinically by examining the velocity of blood being ejected from the ventricles.
The relationship between contractility and stroke volume is pretty straightforward: Increasing contractility causes more blood to be ejected during each cardiac cycle.
Positive inotropic agents (e.g., increased heart rate, sympathetic stimulation, epinephrine) increase contractility and stroke volume.
Heart rate increases only to a certain point: When the heart rate is too high, contractility decreases (Heart is beating too rapidly to develop significant tension during each contraction)
Negative inotropic agents (e.g., certain drugs, hypoxia) decrease contractility.
Afterload
Afterload is the pressure the ventricles must overcome to eject blood into their arteries. It is mainly determined by systemic and pulmonary arterial pressures.
Increased afterload (e.g., hypertension) reduces stroke volume and increases end-systolic volume (ESV). (Ventricular pressure must be greater to exceed the pressure in arterial pulmonary and systemic vessels and open the semilunar valves)
Decreased afterload facilitates ventricular ejection and increases stroke volume.
How Changes in Preload, Contractility, and Afterload Affect Stroke Volume
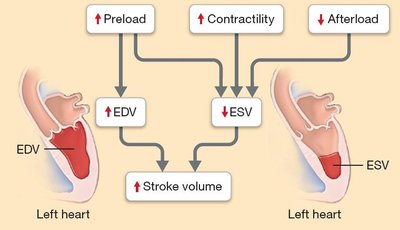
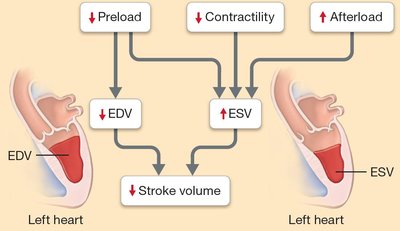
Alterations in preload, contractility, and afterload have direct effects on EDV, ESV, and ultimately stroke volume.
High preload and contractility with low afterload result in high stroke volume and low ESV.
Low preload and contractility with high afterload result in low stroke volume and high ESV.
Ventricular Hypertrophy
Chronic increases in preload and afterload can lead to ventricular hypertrophy, an adaptive enlargement of the ventricular muscle.
Right ventricular hypertrophy is often due to pulmonary hypertension or respiratory disease.
Left ventricular hypertrophy is commonly caused by systemic hypertension.
While initially compensatory, excessive hypertrophy reduces ventricular lumen and filling, increasing the risk of heart failure.
Factors Influencing Heart Rate
Heart rate is primarily determined by the rate of action potential generation in the sinoatrial (SA) node, modulated by chronotropic agents.
Factors that influence the rate at which the SA node depolarizes are known as chronotropic agents
Positive chronotropic agents: Increase heart rate (e.g., sympathetic stimulation, epinephrine, elevated body temperature).
Negative chronotropic agents: Decrease heart rate (e.g., parasympathetic stimulation, acetylcholine, decreased body temperature).
Regulation of Cardiac Output
Cardiac output is regulated by both the nervous and endocrine systems to meet the metabolic demands of the body.
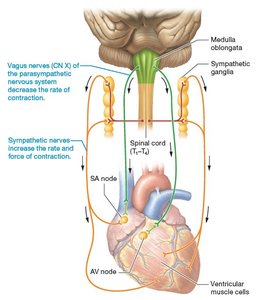
Sympathetic Nervous System: Increases heart rate and contractility via norepinephrine release.
They increase the heart rate by making the SA node fire faster (180-200bpm)
Cause more calcium ions to enter the cardiac muscle cell through calcium ion channels
Unable to control the strength of contraction through recruitment, controls through number of calcium ions that enter the cardiac muscle.
Parasympathetic Nervous System: Decreases heart rate via acetylcholine release from the vagus nerve.
Acetylcholine primarily affects the SA node, decreasing its rate of action potential generation, although it also slows the rate of conduction through the AV node.
Reduces ventricular contractility due to mild negative inotropic effects.
Hormonal Regulation: (positive inotropic and chronotropic agents) Epinephrine, norepinephrine, thyroid hormone, and glucagon increase cardiac output
Aldosterone and antidiuretic hormone increase preload by raising blood volume
Atrial natriuretic peptide decreases preload, reducing cardiac output
Other Factors: Electrolyte concentrations
Body temperature (the SA node fires more rapidly at higher body temperatures and more slowly at lower body temperatures)
Age (younger children and the elderly often have a higher resting heart rate, whereas trained athletes often have a much lower resting heart rate)
Physical fitness also influence cardiac output (exercise increases the stroke volume, so for the body to maintain a constant cardiac output, the heart rate must decrease)

Heart Failure
Heart failure is a condition in which the heart cannot pump sufficient blood to meet the body's needs. It is often caused by reduced contractility, myocardial infarction, valvular disease, or cardiomyopathy.
Left ventricular failure: Leads to pulmonary congestion (blood often backs up within the pulmonary circuit),and pulmonary edema (driving fluid out of the pulmonary capillaries and into the lungs due to blood back up/pressure)
Right ventricular failure: Causes systemic congestion and peripheral edema, especially in the lower extremities.
Exacerbated by the fact that the kidneys retain excess fluid during heart failure
Treatment: Aims to increase cardiac output through lifestyle modifications, medications (to reduce preload, increase contractility, or decrease afterload), and in severe cases, devices or transplantation.
