 Back
BackCardiac Output, Heart Rate, and Stroke Volume: Regulation and Clinical Aspects
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Cardiac Output, Heart Rate, and Stroke Volume
Mechanical Events of the Heart
The cardiac cycle describes the sequence of mechanical and electrical events that repeat with every heartbeat. It includes periods of contraction (systole) and relaxation (diastole) in the atria and ventricles.
Dicrotic notch: The brief rise in aortic pressure caused by backflow of blood rebounding off the closed aortic valve.
Filling of atria: During ventricular systole, the atria fill with blood. When atrial pressure exceeds ventricular pressure, the atrioventricular (AV) valves open, starting the cycle again.
Typical values: The heart beats about 75 times per minute. The cardiac cycle lasts about 0.8 seconds (atrial systole: 0.1 s, ventricular systole: 0.3 s, quiescent period: 0.4 s).
Blood flow: Blood moves through the heart due to pressure changes and flows down a pressure gradient through available openings.
Right vs. left heart: Both sides function similarly except for pressure differences (Pulmonary artery: 24/10 mm Hg; Aorta: 120/80 mm Hg).
Regulation of Cardiac Output (CO)
Cardiac output is the amount of blood pumped by each ventricle per minute. It is a key measure of heart function and is regulated by heart rate (HR) and stroke volume (SV).
Formula:
Example: At rest,
Maximal CO: 4–5 times resting CO in nonathletes (20–25 L/min in athletes).
Cardiac reserve: Difference between resting and maximal CO.
CO changes: If HR or SV changes, CO changes accordingly.
Regulation of Stroke Volume (SV)
Stroke volume is the volume of blood pumped out by one ventricle with each beat. It is determined by three main factors: preload, contractility, and afterload.
Formula:
End-diastolic volume (EDV): Volume of blood in ventricle at end of filling (~120 ml).
End-systolic volume (ESV): Volume of blood remaining after contraction (~50 ml).
Normal SV:

Preload
Preload is the degree of stretch of cardiac muscle cells before contraction. It is directly related to venous return (the amount of blood returning to the heart).
Increased preload increases SV (Frank-Starling law of the heart).
Venous return is enhanced by exercise and increased ventricular filling time.
Contractility
Contractility refers to the contractile strength at a given muscle length, independent of muscle stretch and EDV.
Increased by sympathetic stimulation (epinephrine, norepinephrine), thyroxine, glucagon, digitalis, and high extracellular Ca2+.
Decreased by acidosis, excess K+, and calcium channel blockers.
Increased contractility lowers ESV.
Afterload
Afterload is the pressure that ventricles must overcome to eject blood. It is mainly determined by arterial blood pressure.
Aortic pressure: ~80 mm Hg; Pulmonary trunk pressure: ~10 mm Hg.
Increased afterload (e.g., hypertension) increases ESV and reduces SV.
Regulation of Heart Rate (HR)
Heart rate is regulated by autonomic nervous system input, chemicals, and other factors.
Positive chronotropic factors: Increase HR (e.g., sympathetic stimulation, epinephrine).
Negative chronotropic factors: Decrease HR (e.g., parasympathetic stimulation, acetylcholine).
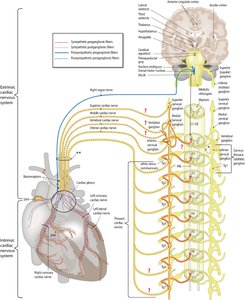
Autonomic Nervous System Regulation
The sympathetic nervous system increases HR and contractility, while the parasympathetic system (vagus nerve) decreases HR.
Sympathetic activation releases norepinephrine, increasing SA node firing and contractility.
Parasympathetic activation releases acetylcholine, hyperpolarizing pacemaker cells and slowing HR.
Baroreceptors respond to changes in blood pressure, influencing HR via reflexes.
Atrial (Bainbridge) reflex increases HR in response to increased venous return and atrial filling.
Chemical Regulation
Hormones: Epinephrine and thyroxine increase HR and contractility.
Ions: Proper intra- and extracellular concentrations of Ca2+ and K+ are essential for normal heart function. Imbalances can cause arrhythmias or cardiac arrest.
Other Factors Affecting Heart Rate
Age: Fetal HR is fastest; declines with age.
Gender: Females generally have higher HR than males.
Exercise: Increases HR; trained athletes may have lower resting HR.
Body temperature: HR increases with temperature.
Clinical Conditions Related to Cardiac Output and Heart Rate
Tachycardia: Abnormally fast HR (>100 beats/min); may lead to fibrillation.
Bradycardia: Abnormally slow HR (<60 beats/min); may be normal in athletes or result from low temperature, drugs, or parasympathetic activation.
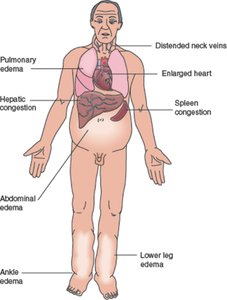
Homeostatic Imbalances of Cardiac Output
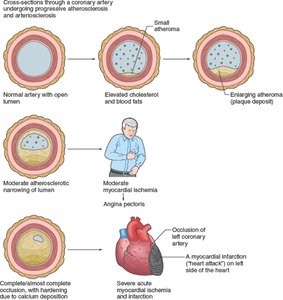
Congestive heart failure (CHF): Progressive condition where CO is too low to meet tissue needs. Causes include coronary atherosclerosis, persistent high blood pressure, multiple myocardial infarcts, and dilated cardiomyopathy (DCM).
Left-sided failure: Results in pulmonary congestion (blood backs up in lungs).
Right-sided failure: Results in peripheral congestion (blood pools in body organs, causing edema).
Treatment includes fluid removal, drugs to reduce afterload, and drugs to increase contractility.
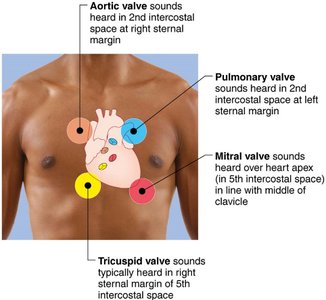
Heart Sounds and Murmurs
Heart sounds are produced by the closing of heart valves. Abnormal sounds (murmurs) may indicate valve problems.
First sound (lub): Closing of AV valves at the beginning of ventricular systole.
Second sound (dup): Closing of SL valves at the beginning of ventricular diastole.
Heart murmurs: Abnormal sounds due to incompetent (leaky) or stenotic (narrowed) valves.
Developmental Aspects of the Heart
Embryonic Development
The human heart develops from mesoderm and begins as two endothelial tubes that fuse to form a single pumping chamber by day 22. The heart tube bends and partitions to form a four-chambered heart by day 35.

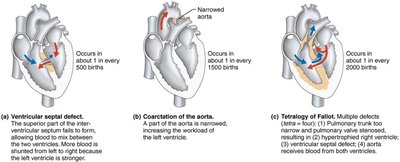
Congenital Heart Defects
Congenital heart defects are the most common birth defects and are usually corrected with surgery. They include:
Mixing of oxygen-poor and oxygen-rich blood: e.g., septal defects.
Narrowed valves or vessels: e.g., coarctation of the aorta.
Tetralogy of Fallot: Combination of four defects causing increased workload on the heart.
Age-Related Changes Affecting the Heart
Regular exercise helps maintain heart health.
Age-related changes include sclerosis and thickening of valve flaps (leading to murmurs), decline in cardiac reserve, fibrosis of cardiac muscle (causing arrhythmias), and atherosclerosis (narrowing of arteries due to fat deposits).
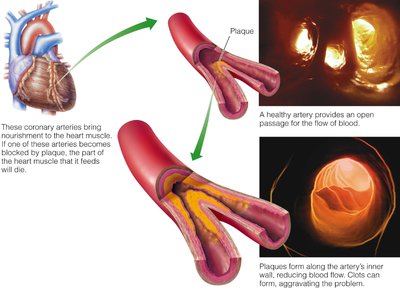
Additional info: Maintaining a healthy diet and regular physical activity can help prevent age-related cardiac changes and reduce the risk of atherosclerosis and heart disease.
