 Back
BackChapter 13: The Peripheral Nervous System – Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Peripheral Nervous System (PNS)
Organization of the Nervous System
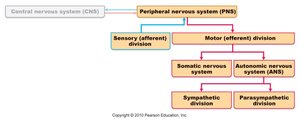
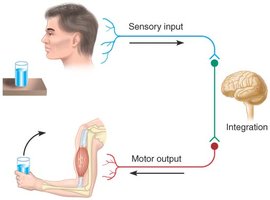
The nervous system is divided into the central nervous system (CNS) and the peripheral nervous system (PNS). The PNS connects the CNS to limbs and organs, serving as a communication relay. It is further divided into sensory (afferent) and motor (efferent) divisions. The motor division includes the somatic nervous system (voluntary control of skeletal muscles) and the autonomic nervous system (involuntary control of smooth muscle, cardiac muscle, and glands).
Sensory Receptors
Classification by Stimulus Detected
Sensory receptors are specialized to respond to changes in their environment (stimuli). They are classified by the type of stimulus they detect:
Mechanoreceptors: Detect mechanical pressure or stretch.
Thermoreceptors: Detect changes in temperature.
Photoreceptors: Detect light (e.g., in the retina).
Chemoreceptors: Detect chemicals in solution (e.g., taste, smell, blood chemistry).
Nociceptors: Detect pain from potentially damaging stimuli.
Classification by Location
Receptors are also classified by their location relative to the stimulus:
Exteroceptors: Detect stimuli from outside the body (e.g., touch, pressure, pain, temperature, special senses).
Interoceptors (Visceroceptors): Detect stimuli within the body (e.g., from blood vessels, internal organs).
Proprioceptors: Detect stretch and position in muscles, tendons, joints, and ligaments.
Classification by Structural Complexity
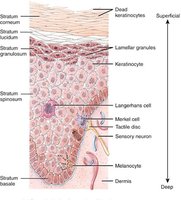
Sensory receptors can be structurally simple or complex:
Unencapsulated (Free) Nerve Endings: Detect temperature, pain, and pressure. Found throughout the body, especially in epithelial and connective tissues.
Encapsulated Nerve Endings: Dendrite endings surrounded by connective tissue, specialized for pressure and stretch (e.g., Meissner's corpuscles, Pacinian corpuscles).
Sensory Receptor Physiology
Stimulation of a receptor produces a graded potential, which, if strong enough, triggers an action potential. The frequency of action potentials encodes the strength of the stimulus. Sensory adaptation refers to a decrease in sensitivity during a constant stimulus. Tonic receptors (e.g., nociceptors, proprioceptors) adapt slowly or not at all, maintaining a sustained response.

Pain and Visceral Sensation
The Pain Response
Pain is a protective sensation produced by tissue-damaging or potentially damaging stimuli. It elicits sensory, autonomic, and emotional responses. Pain perception is influenced by past experiences and emotional state. Hyperalgesia is an increased sensitivity to pain.

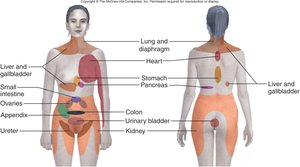
Visceral Pain and Referred Pain
Visceral pain originates in internal organs but is often perceived as coming from the body surface, a phenomenon known as referred pain. This occurs because visceral and somatic sensory fibers converge on the same spinal neurons.
Nerves and Nerve Structure
Definition and Types of Nerves
Nerves are bundles of axons in the PNS (called tracts in the CNS). Most nerves are mixed, containing both sensory and motor fibers.
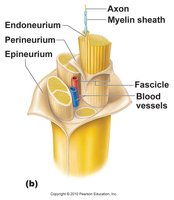
Nerve Structure
Nerves are organized into fascicles, each surrounded by connective tissue layers:
Endoneurium: Surrounds individual nerve fibers (axons).
Perineurium: Surrounds each fascicle (bundle of axons).
Epineurium: Encloses the entire nerve.

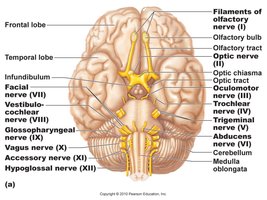
Cranial Nerves
Overview and Classification
There are 12 pairs of cranial nerves, primarily innervating the head and neck. Each is numbered (I–XII) and named. Some are purely sensory, some motor, and some mixed.
Number | Name | Type | Main Function |
|---|---|---|---|
I | Olfactory | Sensory | Smell |
II | Optic | Sensory | Vision |
III | Oculomotor | Motor | Eye movement, pupil constriction |
IV | Trochlear | Motor | Eye movement |
V | Trigeminal | Mixed | Sensory to face, motor to chewing muscles |
VI | Abducens | Motor | Eye movement |
VII | Facial | Mixed | Facial expression, taste, glands |
VIII | Vestibulocochlear | Sensory | Hearing, balance |
IX | Glossopharyngeal | Mixed | Taste, swallowing, salivation |
X | Vagus | Mixed | Viscera sensation, motor to heart, GI tract |
XI | Accessory | Motor | Head and shoulder movement |
XII | Hypoglossal | Motor | Tongue movement |
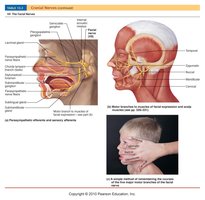
Clinical Relevance: Bell's Palsy
Bell's palsy is a disorder of the facial nerve (CN VII), often due to viral infection, resulting in facial muscle weakness or paralysis.
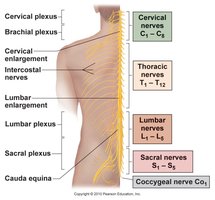
Spinal Nerves and Plexuses
Spinal Nerve Organization
There are 31 pairs of spinal nerves, named for their region of emergence:
8 cervical
12 thoracic
5 lumbar
5 sacral
1 coccygeal
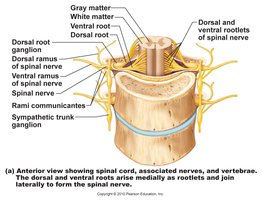
Spinal Nerve Structure
Each spinal nerve forms from the union of a dorsal (sensory) and ventral (motor) root. After exiting the vertebral column, each nerve splits into dorsal and ventral rami. In the cervical, lumbar, and sacral regions, ventral rami form plexuses, redistributing fibers to peripheral nerves.
Major Plexuses and Their Functions
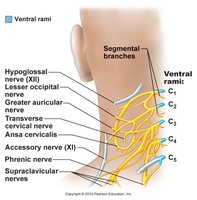
Cervical Plexus (C1–C4): Innervates neck, head, shoulders; phrenic nerve controls diaphragm.
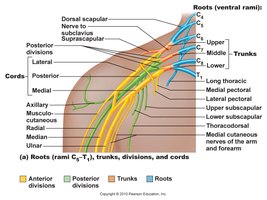
Brachial Plexus (C5–T1): Innervates shoulders, upper limbs; includes median, ulnar, radial nerves.
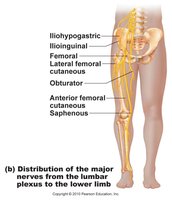
Lumbar Plexus (L1–L4): Innervates abdomen, genitals, anterior thigh; femoral nerve controls thigh flexors.
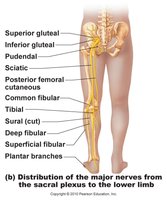
Sacral Plexus (L4–S4): Innervates buttock, lower limb; sciatic nerve is the largest branch.
Motor Endings and Reflex Activity
Motor Endings
Somatic motor neurons release acetylcholine (ACh) at neuromuscular junctions, causing skeletal muscle contraction. Autonomic motor neurons release ACh or norepinephrine (NE) at varicosities, affecting smooth muscle and glands.
Reflexes
Reflexes are rapid, predictable, involuntary responses to stimuli, designed to protect the body. Somatic reflexes involve skeletal muscle; autonomic reflexes involve smooth muscle, cardiac muscle, or glands. Reflexes are important clinically, as abnormal reflexes may indicate nervous system damage.
Reflex Arc
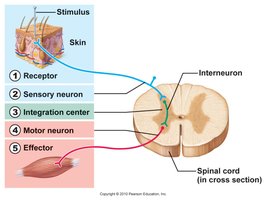
The basic pathway of a reflex (reflex arc) includes:
Receptor
Sensory neuron
Integration center (spinal cord or brain)
Motor neuron
Effector (muscle or gland)
Example: The knee-jerk (patellar) reflex is a classic somatic reflex used in clinical exams to assess nervous system function.
Additional info: Reflexes can be monosynaptic (single synapse, e.g., stretch reflex) or polysynaptic (multiple synapses, e.g., withdrawal reflex).
