 Back
BackChapter 16: Pulmonary Ventilation – Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Pulmonary Ventilation
Overview of Respiration
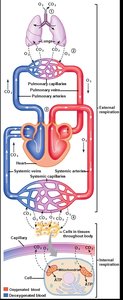
Respiration is the process by which oxygen is delivered to body tissues and carbon dioxide is removed. It involves both external and internal (cellular) respiration. External respiration refers to the exchange of gases between the atmosphere and the blood, while internal respiration refers to the use of oxygen by mitochondria to generate ATP and the production of carbon dioxide as a waste product.
External Respiration: Exchange of O2 and CO2 between the atmosphere and blood.
Internal Respiration: Cellular utilization of O2 and production of CO2.
Functions of the Respiratory System
Beyond gas exchange, the respiratory system plays several vital roles:
Acid-base balance: Regulates blood pH by controlling CO2 exhalation.
Vocalization: Air movement through the larynx enables speech.
Defense: Traps and removes pathogens and particles.
Water and heat loss: Facilitates evaporative cooling and moisture loss.
Venous return: The respiratory pump enhances blood flow back to the heart.
Anatomy of the Respiratory System
Upper Airways and Respiratory Tract
The respiratory system is divided into the upper airways and the respiratory tract. The upper airways include the nasal and oral cavities, pharynx, and larynx. The respiratory tract is further divided into the conducting and respiratory zones.
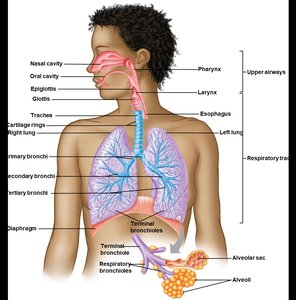
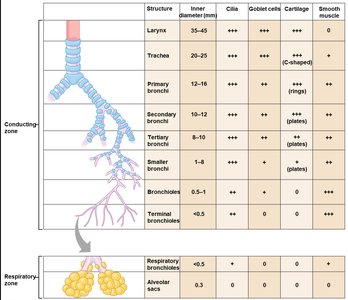
Conducting and Respiratory Zones
The conducting zone consists of structures that transport air but do not participate in gas exchange (e.g., trachea, bronchi, bronchioles). The respiratory zone includes structures where gas exchange occurs (respiratory bronchioles, alveolar ducts, alveoli).
Structure | Inner Diameter (mm) | Cilia | Goblet Cells | Cartilage | Smooth Muscle |
|---|---|---|---|---|---|
Larynx | 35-45 | +++ | +++ | +++ | 0 |
Trachea | 20-25 | +++ | +++ | +++ (C-shaped) | + |
Primary bronchi | 12-16 | +++ | +++ | +++ (rings) | ++ |
Secondary bronchi | 10-12 | +++ | +++ | +++ (plates) | ++ |
Tertiary bronchi | 8-10 | +++ | ++ | ++ (plates) | ++ |
Smaller bronchi | 1-8 | ++ | + | + (plates) | +++ |
Bronchioles | 0.5-1 | + | 0 | 0 | +++ |
Terminal bronchioles | <0.5 | 0 | 0 | 0 | +++ |
Respiratory bronchioles | <0.5 | 0 | 0 | 0 | 0 |
Alveolar sacs | 0.3 | 0 | 0 | 0 | 0 |
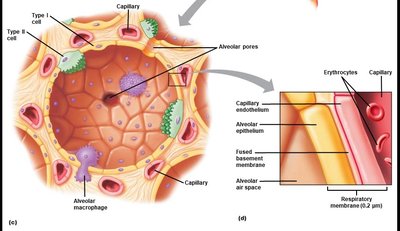
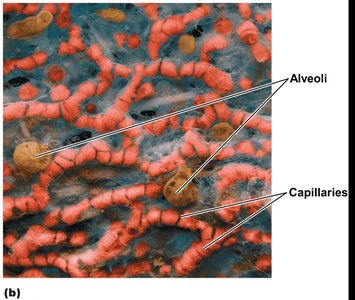
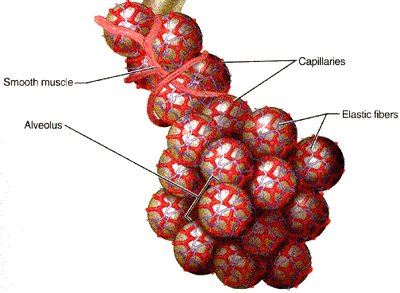
Alveoli and the Respiratory Membrane
Alveoli are tiny air sacs where gas exchange occurs. They are surrounded by capillaries and have a thin respiratory membrane to facilitate rapid diffusion of gases. The membrane consists of alveolar epithelium, fused basement membrane, and capillary endothelium.
Type I cells: Form the structure of the alveolar wall.
Type II cells: Secrete surfactant to reduce surface tension.
Alveolar macrophages: Remove debris and pathogens.
Mechanics of Breathing
The Pleura and Thoracic Cavity
Each lung is surrounded by a double-layered pleural sac. The pleural cavity contains serous fluid, which lubricates and reduces friction. The negative pressure in the pleural space (intrapleural pressure) keeps the lungs partially expanded.
Visceral pleura: Adheres to the lung surface.
Parietal pleura: Lines the chest wall and diaphragm.
Pleural fluid: Provides lubrication and surface tension.
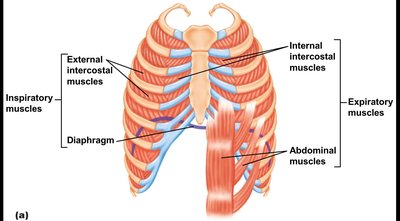
Muscles of Respiration
Breathing is driven by the coordinated action of inspiratory and expiratory muscles:
Inspiration: Diaphragm and external intercostal muscles contract, expanding the thoracic cavity.
Expiration: Usually passive; active expiration involves internal intercostals and abdominal muscles.
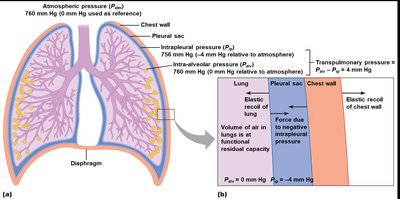
Pulmonary Pressures and Elastic Recoil
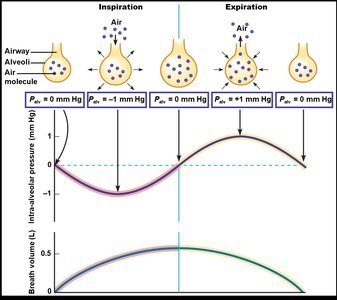
Airflow is driven by pressure gradients between the atmosphere and alveoli. Key pressures include:
Atmospheric pressure (Patm): Pressure of air outside the body (reference: 0 mm Hg).
Intra-alveolar pressure (Palv): Pressure within the alveoli; changes during breathing.
Intrapleural pressure (Pip): Pressure within the pleural cavity; always negative relative to Patm.
Transpulmonary pressure: ; keeps lungs inflated.
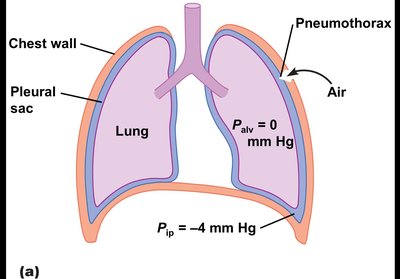
Pneumothorax
If intrapleural pressure equilibrates with atmospheric pressure (e.g., due to a puncture), the lung collapses (pneumothorax) because the elastic recoil of the lung is unopposed.
Air Flow and Pressure Gradients
Airflow () is determined by the pressure difference between the atmosphere and alveoli, divided by airway resistance ():
During inspiration, Palv < Patm; during expiration, Palv > Patm.
Neural Control of Ventilation
Breathing is regulated by neural input to the respiratory muscles. The sequence involves neural stimulation, muscle contraction, thoracic expansion, decreased intrapleural pressure, increased transpulmonary pressure, and airflow into the alveoli.
Factors Affecting Pulmonary Ventilation
Lung Compliance
Lung compliance is the ease with which the lungs can expand. It is defined as:
High compliance: Lungs expand easily with little pressure change.
Low compliance: More muscular work is required to expand the lungs.
Compliance depends on lung elasticity and alveolar surface tension.
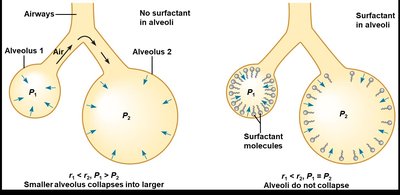
Surface Tension and Surfactant
The thin film of water lining the alveoli creates surface tension, which opposes lung expansion. According to LaPlace’s Law:
where is the pressure to prevent collapse, is surface tension, and is alveolar radius. Pulmonary surfactant, secreted by type II cells, reduces surface tension, increases compliance, and prevents alveolar collapse.
Airway Resistance
Airway resistance is influenced by airway diameter, smooth muscle tone, and mucus production. Increased resistance requires a greater pressure gradient to maintain airflow.
Bronchoconstriction: Decreases airway diameter, increases resistance (e.g., asthma, histamine release).
Bronchodilation: Increases airway diameter, decreases resistance (e.g., sympathetic stimulation, high CO2).
Clinical Assessment of Pulmonary Function
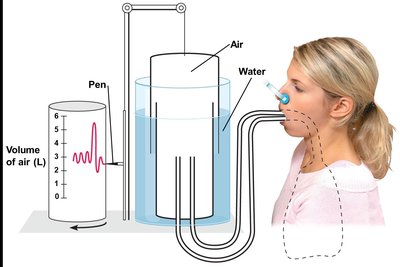
Spirometry and Lung Volumes
Spirometry measures lung volumes and capacities, which are essential for diagnosing respiratory diseases.
Tidal Volume (VT): Volume of air inhaled/exhaled in a normal breath (~500 mL).
Inspiratory Reserve Volume (IRV): Maximum volume inhaled above VT (~3000 mL).
Expiratory Reserve Volume (ERV): Maximum volume exhaled below VT (~1000 mL).
Residual Volume (RV): Volume remaining after maximal exhalation (~1200 mL).
Lung capacities are combinations of these volumes:
Inspiratory Capacity (IC):
Vital Capacity (VC):
Functional Residual Capacity (FRC):
Total Lung Capacity (TLC):
Minute and Alveolar Ventilation
Minute ventilation (VE) is the total volume of air entering or leaving the lungs per minute:
Alveolar ventilation (VA) accounts for dead space (air not involved in gas exchange):
Pulmonary Diseases
Obstructive Diseases: Increased airway resistance (e.g., asthma, COPD). Characterized by increased RV, FRC, and TLC; FEV1/FVC ratio is reduced.
Restrictive Diseases: Decreased lung compliance (e.g., fibrosis). Characterized by reduced TLC and VC; FEV1/FVC ratio may be normal or increased.
Forced Vital Capacity (FVC): Maximum volume exhaled forcefully after maximal inspiration. Forced Expiratory Volume in 1 second (FEV1): Volume exhaled in the first second of FVC maneuver. FEV1/FVC ratio: Used to differentiate between obstructive and restrictive diseases.
Summary Table: Lung Volumes and Capacities
Parameter | Definition | Normal Value (mL) |
|---|---|---|
VT (Tidal Volume) | Normal breath | 500 |
IRV | Maximal inspiration above VT | 3000 |
ERV | Maximal expiration below VT | 1000 |
RV | Volume after maximal expiration | 1200 |
IC | VT + IRV | 3500 |
VC | VT + IRV + ERV | 4500 |
FRC | ERV + RV | 2200 |
TLC | VT + IRV + ERV + RV | 5700 |
Study tip: Be able to define and explain the functional significance of these lung volumes and capacities.
