 Back
BackChapter 18: The Cardiovascular System – Heart Anatomy and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Cardiovascular System: The Heart
Pulmonary and Systemic Circuits
The heart functions as a dual pump, circulating blood through two distinct circuits: the pulmonary and systemic circuits. The right side of the heart receives oxygen-poor blood from the body and pumps it to the lungs for gas exchange, while the left side receives oxygen-rich blood from the lungs and pumps it throughout the body.
Pulmonary Circuit: Carries blood from the right ventricle to the lungs and back to the left atrium.
Systemic Circuit: Carries blood from the left ventricle to the body tissues and back to the right atrium.
Key Point: Both circuits pump equal volumes of blood, but the systemic circuit operates under higher pressure and resistance.
Example: Oxygen-poor blood enters the right atrium, passes through the right ventricle, and is sent to the lungs; oxygen-rich blood returns to the left atrium, passes through the left ventricle, and is sent to the body.

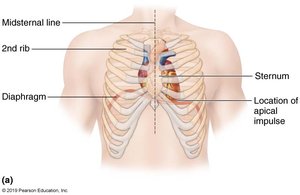
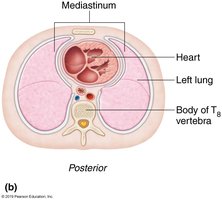
Size, Location, and Orientation of the Heart
The heart is roughly the size of a fist and weighs less than one pound. It is located in the mediastinum, between the second rib and fifth intercostal space, on the superior surface of the diaphragm. Two-thirds of the heart lies to the left of the midsternal line, anterior to the vertebral column and posterior to the sternum.
Base: Leans toward the right shoulder.
Apex: Points toward the left hip; apical impulse can be palpated between the fifth and sixth ribs, just below the left nipple.
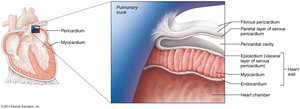
Coverings of the Heart: The Pericardium
The heart is enclosed in a double-walled sac called the pericardium. The superficial fibrous pericardium protects and anchors the heart, while the deep serous pericardium consists of two layers (parietal and visceral/epicardium) separated by a fluid-filled pericardial cavity that reduces friction during heart movements.
Fibrous Pericardium: Protects, anchors, and prevents overfilling.
Serous Pericardium: Parietal layer lines the fibrous pericardium; visceral layer (epicardium) covers the heart.
Pericardial Cavity: Contains serous fluid to decrease friction.
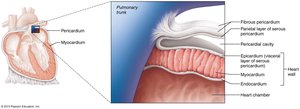
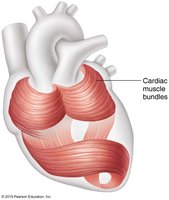
Layers of the Heart Wall
The heart wall consists of three layers: epicardium, myocardium, and endocardium. The myocardium is composed of spiral and circular bundles of cardiac muscle cells, supported by the cardiac skeleton (connective tissue network).
Epicardium: Visceral layer of serous pericardium.
Myocardium: Contractile cardiac muscle; responsible for pumping action.
Cardiac Skeleton: Anchors muscle fibers, supports vessels and valves, limits spread of action potentials.
Endocardium: Innermost layer; continuous with endothelial lining of blood vessels.
Chambers and Associated Great Vessels
Internal and Surface Features
The heart has four chambers: two superior atria and two inferior ventricles. The interatrial septum separates the atria, while the interventricular septum separates the ventricles. Surface features include the coronary sulcus, anterior and posterior interventricular sulci.
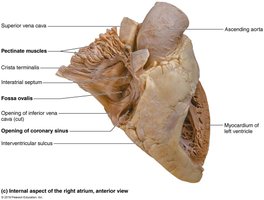
Fossa Ovalis: Remnant of fetal foramen ovale.
Coronary Sulcus: Encircles junction of atria and ventricles.
Anterior/Posterior Interventricular Sulcus: Landmarks for septum position.
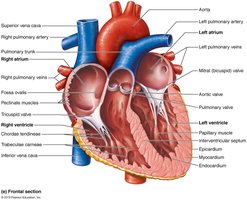
Atria: The Receiving Chambers
Atria are small, thin-walled chambers that receive blood. The right atrium receives deoxygenated blood from the body via the superior and inferior vena cava and coronary sinus. The left atrium receives oxygenated blood from the lungs via four pulmonary veins.
Auricles: Increase atrial volume.
Pectinate Muscles: Ridges in the right atrium and auricles.
Crista Terminalis: Separates smooth and ridged regions in right atrium.
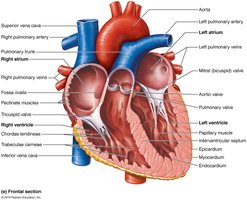
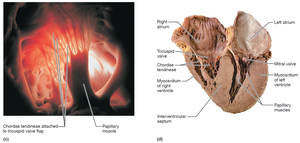
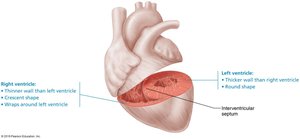
Ventricles: The Discharging Chambers
Ventricles are thick-walled chambers responsible for pumping blood out of the heart. The right ventricle pumps blood into the pulmonary trunk, while the left ventricle pumps blood into the aorta. Both contain trabeculae carneae and papillary muscles, which anchor the chordae tendineae of the heart valves.
Right Ventricle: Most of anterior surface; pumps to pulmonary circuit.
Left Ventricle: Posteroinferior surface; pumps to systemic circuit.
Trabeculae Carneae: Irregular ridges of muscle.
Papillary Muscles: Anchor valve flaps.
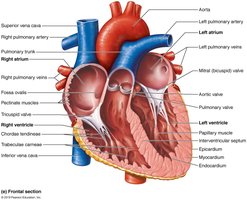
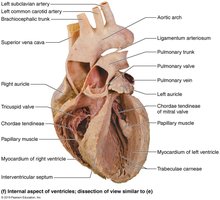
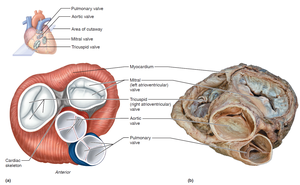
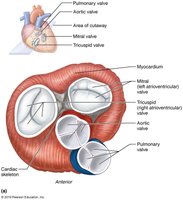
Heart Valves
Types and Functions
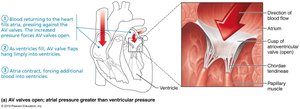
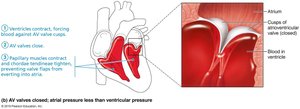
Heart valves ensure unidirectional blood flow and open/close in response to pressure changes. There are two main types: atrioventricular (AV) valves between atria and ventricles, and semilunar (SL) valves between ventricles and major arteries.
AV Valves: Tricuspid (right) and mitral/bicuspid (left); prevent backflow into atria.
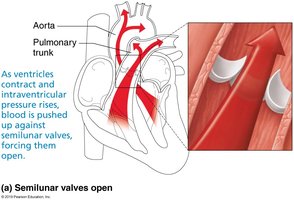
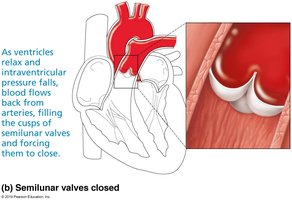
SL Valves: Pulmonary (right) and aortic (left); prevent backflow into ventricles.
Chordae Tendineae: Anchor AV valve cusps to papillary muscles.
Clinical Imbalances
Incompetent Valve: Blood backflows, requiring repeated pumping.
Valvular Stenosis: Stiff flaps constrict opening, increasing cardiac workload.
Treatment: Replacement with mechanical, animal, or cadaver valves.
Pathway of Blood Through the Heart
Right Side (Pulmonary Circuit)
Superior vena cava, inferior vena cava, and coronary sinus → right atrium → tricuspid valve → right ventricle → pulmonary semilunar valve → pulmonary trunk → pulmonary arteries → lungs
Left Side (Systemic Circuit)
Four pulmonary veins → left atrium → mitral valve → left ventricle → aortic semilunar valve → aorta → systemic circulation

Ventricular Anatomy and Circuit Differences
Pulmonary Circuit: Short, low-pressure.
Systemic Circuit: Long, high-friction; left ventricle walls are three times thicker than right.
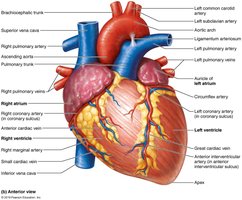
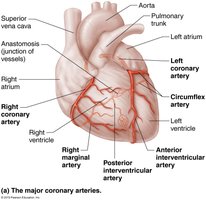
Coronary Circulation
Coronary Arteries
Coronary circulation supplies blood to the heart muscle itself. The left and right coronary arteries arise from the base of the aorta and encircle the heart in the coronary sulcus. They branch to supply different regions of the heart and contain anastomoses for collateral circulation.
Left Coronary Artery: Branches into anterior interventricular and circumflex arteries.
Right Coronary Artery: Branches into right marginal and posterior interventricular arteries.
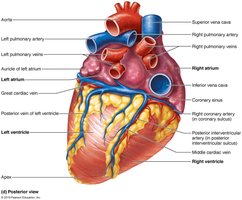
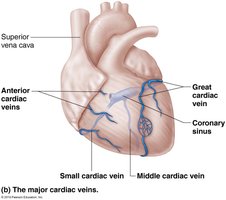
Coronary Veins
Cardiac veins collect blood from capillary beds and merge to form the coronary sinus, which empties into the right atrium. Major veins include the great cardiac vein, middle cardiac vein, small cardiac vein, and several anterior cardiac veins.
Microscopic Anatomy of Cardiac Muscle
Cardiac Muscle Cell Structure
Cardiac muscle cells are striated, short, branched, and interconnected, typically with one central nucleus. They contain numerous large mitochondria for resistance to fatigue and are organized into sarcomeres with Z discs, A bands, and I bands.
T Tubules: Wider, less numerous; enter at Z disc.
Sarcoplasmic Reticulum: Simpler than in skeletal muscle; no triads.
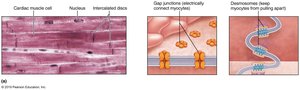
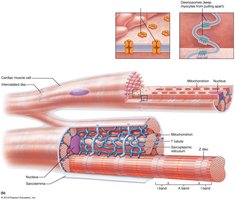
Intercalated Discs and Functional Syncytium
Intercalated discs connect cardiac cells via desmosomes (prevent separation during contraction) and gap junctions (allow ion passage and electrical coupling). This enables the heart to function as a single coordinated unit (functional syncytium).
Comparison: Skeletal vs. Cardiac Muscle Physiology
Key Differences
Self-Excitability: Some cardiac cells are pacemaker cells, capable of spontaneous depolarization.
Contraction: Cardiac muscle contracts as a unit; skeletal muscle contracts independently.
Calcium Source: Cardiac muscle uses both sarcoplasmic reticulum and extracellular Ca2+; skeletal muscle uses only sarcoplasmic reticulum.
Refractory Period: Cardiac muscle has a longer absolute refractory period, preventing tetanic contractions.
ATP Supply: Cardiac muscle relies almost exclusively on aerobic respiration due to abundant mitochondria.
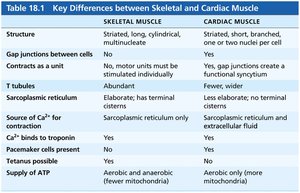
Feature | Skeletal Muscle | Cardiac Muscle |
|---|---|---|
Structure | Striated, long, cylindrical, multinucleate | Striated, short, branched, one or two nuclei per cell |
Gap Junctions | No | Yes |
Contracts as a Unit | No | Yes |
T Tubules | Abundant | Fewer |
Sarcoplasmic Reticulum | Elaborate | Less elaborate |
Source of Ca2+ | Sarcoplasmic reticulum | Sarcoplasmic reticulum and extracellular fluid |
Ca2+ binds to troponin | Yes | Yes |
Pace Maker Cells | No | Yes |
Tetany Possible | Yes | No |
ATP Supply | Aerobic and anaerobic | Aerobic only (more mitochondria) |
Summary
The heart is a complex organ with specialized anatomy and physiology, ensuring efficient circulation of blood through the pulmonary and systemic circuits. Its unique muscle structure and electrical properties distinguish it from skeletal muscle, enabling continuous, rhythmic contractions essential for life.
