 Back
BackChapter 18: The Cardiovascular System – The Heart
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Heart: Structure and Function
Size, Location, and Orientation of the Heart
The heart is a muscular organ located in the mediastinum of the thoracic cavity. Its base is positioned superiorly and posteriorly, while the apex points inferiorly and to the left. The heart's orientation allows it to efficiently pump blood throughout the body.
Mediastinum: Central compartment of the thoracic cavity.
Base of heart: Broad, superior portion where major vessels attach.
Apex of heart: Pointed, inferior tip directed toward the left hip.
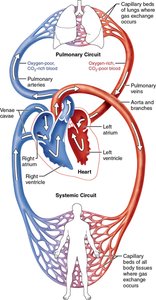
The Pulmonary and Systemic Circuits
The heart functions as two side-by-side pumps, each serving a distinct circulatory circuit:
Pulmonary circuit: Right side of the heart pumps oxygen-poor blood to the lungs for gas exchange.
Systemic circuit: Left side of the heart pumps oxygen-rich blood to the rest of the body.
Coverings and Layers of the Heart
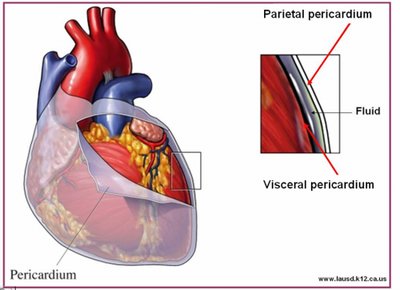
Pericardium: The Heart's Protective Sac
The heart is enclosed in a double-walled sac called the pericardium, which consists of two main layers:
Fibrous pericardium: Superficial, tough connective tissue layer that protects and anchors the heart.
Serous pericardium: Deep, two-layered membrane (parietal and visceral layers) with a fluid-filled cavity that reduces friction during heartbeats.
Clinical Note: Pericarditis and Cardiac Tamponade
Pericarditis is inflammation of the pericardium, causing roughened membrane surfaces and chest pain. Cardiac tamponade occurs when excess fluid accumulates in the pericardial cavity, compressing the heart and impairing its function.

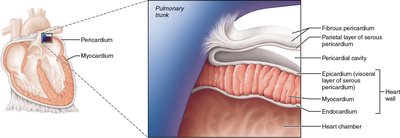
Layers of the Heart Wall
The heart wall is composed of three distinct layers:
Epicardium: Visceral layer of the serous pericardium.
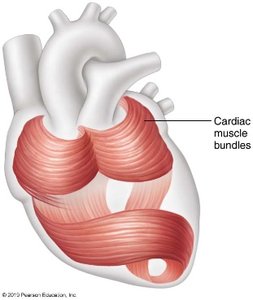
Myocardium: Thick, muscular middle layer responsible for contraction; contains spiral bundles of cardiac muscle cells and the cardiac skeleton (structural support).
Endocardium: Thin, inner lining of the heart chambers and valves.
Gross Anatomy of the Heart
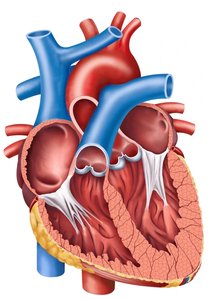
Internal and External Structures
The heart contains four chambers: two atria (upper) and two ventricles (lower). Major vessels include the aorta, pulmonary arteries and veins, and venae cavae. The heart's internal anatomy features valves, septa, and muscle bundles.
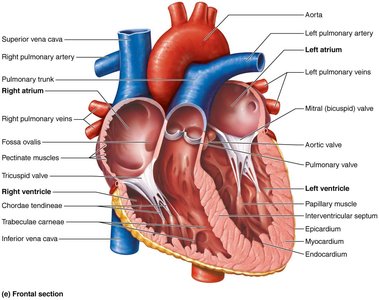
Heart Valves
Types and Functions of Heart Valves
Valves ensure unidirectional blood flow through the heart, preventing backflow:
Atrioventricular (AV) valves: Located between atria and ventricles (tricuspid and bicuspid/mitral valves).
Semilunar (SL) valves: Located between ventricles and major arteries (pulmonary and aortic valves).
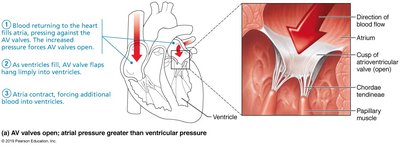
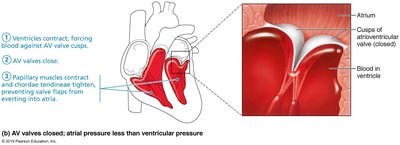
Atrioventricular (AV) Valves
AV valves prevent backflow into the atria when ventricles contract. Chordae tendineae anchor the valve cusps to papillary muscles, ensuring proper closure during contraction.
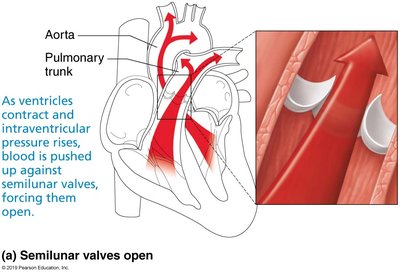
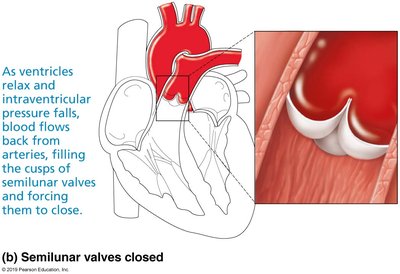
Semilunar (SL) Valves
SL valves prevent backflow from arteries into the ventricles. They open when ventricular pressure rises and close when it falls.
Clinical Note: Valve Disorders
Valve disorders include incompetent/insufficient valves (fail to close properly, causing regurgitation) and valvular stenosis (narrowed valves, increasing workload). Defective valves may be replaced surgically.
Pathway of Blood Through the Heart
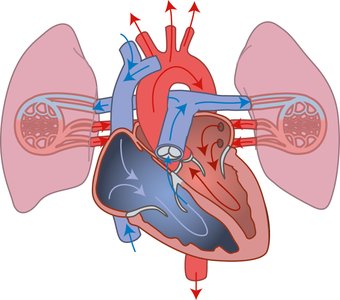
Pulmonary and Systemic Circuits
Blood flows through the heart in a specific sequence, passing through the pulmonary and systemic circuits:
Pulmonary circuit: Right ventricle → pulmonary arteries → lungs → pulmonary veins → left atrium.
Systemic circuit: Left ventricle → aorta → body tissues → venae cavae → right atrium.
Anatomical Differences Between Ventricles
The left ventricle has a thicker wall than the right, reflecting its role in pumping blood throughout the systemic circuit (higher pressure and resistance).
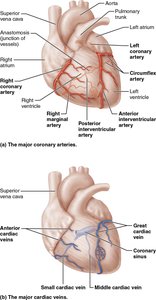
Coronary Circulation
Blood Supply to the Heart
The heart receives its own blood supply via the coronary arteries, which branch from the aorta. The coronary veins collect deoxygenated blood and return it to the right atrium via the coronary sinus.
Clinical Note: Myocardial Ischemia and Infarction
Myocardial ischemia (reduced blood flow) can cause angina pectoris (chest pain). Myocardial infarction (heart attack) results from prolonged blockage, leading to cell death and scar tissue formation.
Cardiac Muscle Fiber Anatomy
Intercalated Discs and Cell Coupling
Cardiac muscle cells are connected by intercalated discs, which contain desmosomes (mechanical strength) and gap junctions (electrical coupling). This allows the heart to contract as a coordinated unit.
Differences Between Skeletal and Cardiac Muscle
Some cardiac muscle cells are self-excitable (pacemaker cells).
Cardiac muscle relies almost exclusively on aerobic respiration.
Heart depolarizes independently of nervous system input.
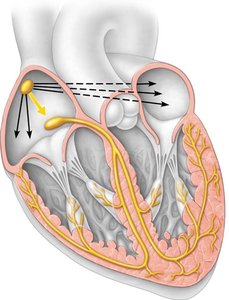
The Intrinsic Conduction System
Setting the Basic Rhythm
The heart's rhythm is set by the intrinsic conduction system, a network of autorhythmic cells that initiate and distribute electrical impulses.
Sinoatrial (SA) node: Pacemaker, initiates heartbeat.
Atrioventricular (AV) node: Delays impulse, allows atrial contraction.
AV bundle (bundle of His): Conducts impulse to ventricles.
Bundle branches: Carry impulse through interventricular septum.
Purkinje fibers: Distribute impulse to ventricular walls.

Clinical Note: Arrhythmias and Fibrillation
Defects in the conduction system can cause arrhythmias (irregular heart rhythms) and fibrillation (rapid, uncoordinated contractions).
Extrinsic Innervation and Regulation of the Heart
Autonomic Nervous System (ANS) Regulation
The ANS modifies heart rate and force of contraction:
Sympathetic stimulation: Increases heart rate and contractility.
Parasympathetic stimulation: Decreases heart rate via the vagus nerve.
Action Potentials in Cardiac Muscle Cells
Cardiac muscle action potentials involve rapid depolarization (Na+ influx), a plateau phase (Ca2+ influx), and repolarization (K+ efflux).
Mechanical Events of the Heart
Systole and Diastole
Systole is the contraction phase, and diastole is the relaxation phase. These events drive blood flow through the heart and into the circulatory system.
Phases of the Cardiac Cycle
Ventricular filling: Blood flows passively into ventricles; atrial contraction completes filling (EDV).
Isovolumetric contraction: Ventricles contract with all valves closed.
Ventricular ejection: Blood is pumped out; remaining volume is ESV.
Heart Sounds
Two main heart sounds (lub-dup) are produced by the closing of AV and SL valves.
Regulation of Cardiac Output
Stroke Volume and Cardiac Output
Stroke volume (SV) is the amount of blood pumped by a ventricle per beat. Cardiac output (CO) is the total volume pumped per minute.
Mathematically:
SV is determined by preload, contractility, and afterload.
Preload: Degree of stretch of cardiac muscle (Frank-Starling law).
Contractility: Force of contraction, influenced by sympathetic stimulation and Ca2+ influx.
Afterload: Pressure the heart must overcome to eject blood.
Regulation of Heart Rate
Heart rate is regulated by the ANS, hormones (epinephrine, thyroxine), ions (Ca2+, K+), age, gender, exercise, and body temperature.
Clinical Notes: Heart Rate and Congenital Defects
Tachycardia and Bradycardia
Tachycardia: Abnormally fast heart rate.
Bradycardia: Abnormally slow heart rate, may affect circulation.
Congenital Heart Defects
Most common birth defects, often corrected surgically. Types include mixing of oxygen-poor and oxygen-rich blood (septal defects) and narrowed valves or vessels.
Career Relevance
Understanding the heart's structure and function is essential for health professionals, including those in athletic training, physical therapy, and medicine. Mastery of this material enables effective diagnosis, treatment, and prevention of cardiovascular disorders.
