 Back
BackChapter 20: The Heart – Anatomy, Physiology, and Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Anatomy of the Heart
Overview of the Cardiovascular System
The cardiovascular system consists of the heart and blood vessels, which together transport blood throughout the body. The heart pumps blood through two main circuits: the pulmonary circuit (to and from the lungs) and the systemic circuit (to and from the rest of the body).
Arteries: Carry blood away from the heart.
Veins: Return blood to the heart.
Capillaries: Smallest vessels where exchange of gases, nutrients, and wastes occurs.

Heart Chambers and Blood Flow
The heart has four chambers:
Right atrium: Receives deoxygenated blood from the systemic circuit.
Right ventricle: Pumps blood into the pulmonary circuit.
Left atrium: Receives oxygenated blood from the pulmonary circuit.
Left ventricle: Pumps blood into the systemic circuit.
The atria contract together, followed by the ventricles contracting together.
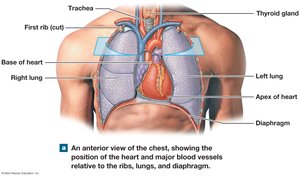
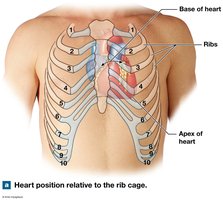
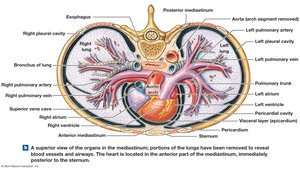
Location and Position of the Heart
The heart is located in the thoracic cavity, posterior to the sternum, between the lungs in the mediastinum. The base is superior, where the great vessels attach, and the apex is inferior and pointed.
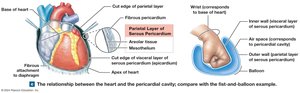
Pericardium and Heart Wall
The pericardium is a double-walled sac that surrounds the heart:
Fibrous pericardium: Outer layer, stabilizes the heart.
Serous pericardium: Inner layer, with parietal and visceral (epicardium) layers.
Pericardial cavity: Space between serous layers, contains lubricating fluid.
Layers of the Heart Wall
Epicardium: Outer layer (visceral pericardium).
Myocardium: Middle, muscular layer responsible for contraction.
Endocardium: Inner layer, lines chambers and valves.
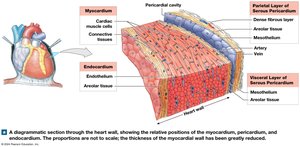
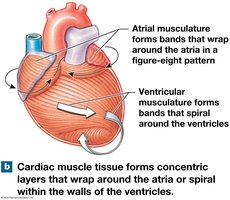
Connective Tissues and Cardiac Skeleton
Connective tissues support cardiac muscle fibers, distribute contraction forces, and provide elasticity. The cardiac skeleton is a framework of dense connective tissue that stabilizes valves and electrically insulates atria from ventricles.
Heart Chambers, Valves, and Great Vessels
The heart's chambers are separated by septa:
Interatrial septum: Between atria.
Interventricular septum: Between ventricles.
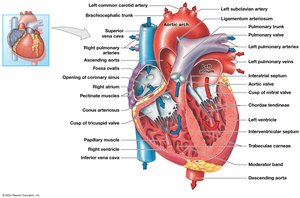
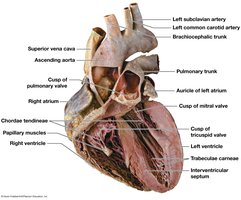
Heart Valves
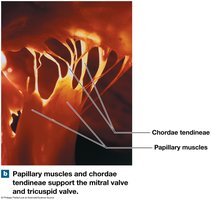
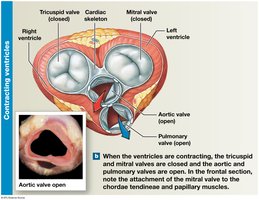
Atrioventricular (AV) valves: Tricuspid (right), Mitral/Bicuspid (left). Prevent backflow into atria.
Semilunar valves: Pulmonary (right), Aortic (left). Prevent backflow into ventricles.
Chordae tendineae and papillary muscles anchor AV valves.

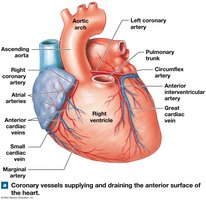
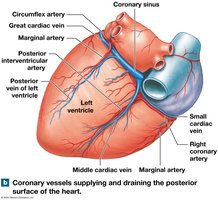
Coronary Circulation
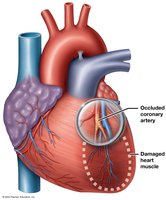
The heart muscle receives blood via the coronary arteries and is drained by cardiac veins. Blockage can lead to ischemia or myocardial infarction (heart attack).
Right coronary artery: Supplies right atrium, parts of both ventricles.
Left coronary artery: Supplies left atrium, left ventricle, interventricular septum.
Great cardiac vein: Drains into the coronary sinus, which empties into the right atrium.
The Conducting System of the Heart
Cardiac Muscle Cell Types
Autorhythmic cells: Pacemaker and conducting cells that initiate and coordinate heartbeat.
Contractile cells: Produce contractions to propel blood.
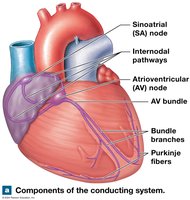
Components of the Conducting System
Sinoatrial (SA) node: Primary pacemaker, located in right atrium.
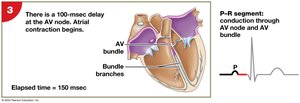
Atrioventricular (AV) node: Junction between atria and ventricles.
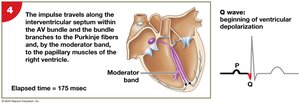
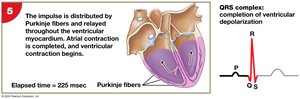
AV bundle, bundle branches, Purkinje fibers: Distribute impulse through ventricles.
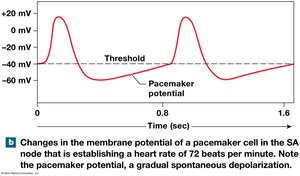
Pacemaker Potential and Heart Rhythm
Pacemaker cells have an unstable resting membrane potential, leading to spontaneous depolarization (pacemaker potential). The SA node sets the basic heart rhythm (sinus rhythm).
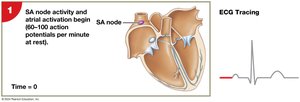
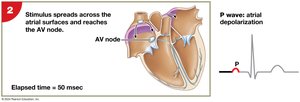
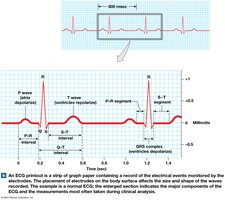
Impulse Conduction and ECG
The electrical impulse travels from the SA node through the atria to the AV node, then through the AV bundle, bundle branches, and Purkinje fibers, causing coordinated contraction. The electrocardiogram (ECG) records these electrical events.
Electrocardiogram (ECG) Features
P wave: Atrial depolarization.
QRS complex: Ventricular depolarization.
T wave: Ventricular repolarization.
Cardiac Arrhythmias
Arrhythmias are disturbances in heart rhythm, such as bradycardia (slow), tachycardia (fast), and ectopic pacemakers (abnormal rhythm sources).


Action Potentials in Cardiac Contractile Cells
Cardiac contractile cells have a unique action potential with three phases:
Rapid depolarization: Influx of Na+.
Plateau: Ca2+ influx maintains depolarization.
Repolarization: K+ efflux restores resting potential.
Refractory Periods
Absolute refractory period: No new action potential possible.
Relative refractory period: Only strong stimulus can trigger action potential.
Role of Calcium Ions
Calcium ions entering during the plateau phase trigger further Ca2+ release from the sarcoplasmic reticulum, essential for contraction. Removal of Ca2+ ends contraction.
The Cardiac Cycle
Phases of the Cardiac Cycle
The cardiac cycle is the period from the start of one heartbeat to the next, including systole (contraction) and diastole (relaxation) of both atria and ventricles.
Atrial systole: Atria contract, filling ventricles.
Ventricular systole: Ventricles contract, ejecting blood.
Ventricular diastole: Ventricles relax and fill passively.
Pressure and Volume Relationships
End-diastolic volume (EDV): Maximum blood in ventricle after diastole (~130 mL).
Stroke volume (SV): Blood ejected per beat (~70–80 mL).
Ejection fraction: Percentage of EDV ejected (~60%).
End-systolic volume (ESV): Blood remaining after contraction (~50 mL).
Heart Sounds
Lubb: AV valves close.
Dupp: Semilunar valves close.
Heart murmur: Abnormal sound due to valve regurgitation.
Cardiac Output and Its Regulation
Cardiac Output (CO)
Cardiac output is the amount of blood pumped by the left ventricle per minute. It is calculated as:
CO = Heart Rate (HR) × Stroke Volume (SV)
Factors Affecting Heart Rate
Autonomic innervation: Sympathetic increases HR, parasympathetic decreases HR.
Cardiac reflexes: Baroreceptors and chemoreceptors monitor blood pressure and gas levels.
Venous return: Increased return increases HR (Bainbridge reflex).
Hormones: Epinephrine, norepinephrine, and thyroid hormone increase HR.
Factors Affecting Stroke Volume
Preload: Degree of ventricular stretch at end of diastole (Frank–Starling principle: more in = more out).
Contractility: Force of contraction at a given preload; increased by sympathetic stimulation and certain hormones.
Afterload: Resistance the ventricle must overcome to eject blood; increased afterload decreases SV.
Summary of Cardiac Output Regulation
Cardiac output is tightly regulated to meet the body's metabolic demands. Both heart rate and stroke volume are adjusted by neural, hormonal, and local factors.
Cardiac Reserve
Cardiac reserve is the difference between resting and maximal cardiac output. Trained athletes have a higher cardiac reserve, but there is a physiological limit due to reduced filling time at very high heart rates.
Clinical Correlations
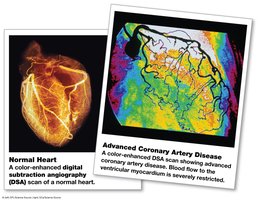
Coronary Artery Disease (CAD) and Myocardial Infarction (MI)
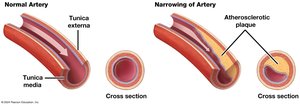
CAD: Blockage of coronary arteries, often due to atherosclerosis, leading to ischemia and angina pectoris.
MI: Heart attack; death of cardiac muscle due to prolonged ischemia.
Diagnosis: ECG, blood tests for cardiac enzymes (troponin T, troponin I, CK-MB).
Treatment: Lifestyle modification, medications, angioplasty, stents, coronary artery bypass graft (CABG).
Term | Definition |
|---|---|
Preload | Degree of stretch of the ventricular myocardium at the end of diastole |
Afterload | Resistance the ventricle must overcome to eject blood |
Contractility | Force of contraction at a given preload |
Stroke Volume (SV) | Volume of blood ejected per beat |
Cardiac Output (CO) | Volume of blood ejected per minute |
Additional info: This guide covers the anatomy, physiology, and clinical aspects of the heart as outlined in a standard college-level Anatomy & Physiology course, focusing on structure, function, regulation, and disease.
