 Back
BackChapter 20: The Heart – Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Heart: Structure, Function, and Physiology
Overview of the Heart and Circulatory Circuits
The heart is a muscular organ responsible for pumping blood throughout the body via two main circuits: the pulmonary circuit and the systemic circuit. These circuits ensure the delivery of oxygen and nutrients to tissues and the removal of waste products.
Pulmonary Circuit: Carries deoxygenated blood from the right side of the heart to the lungs and returns oxygenated blood to the left side of the heart.
Systemic Circuit: Delivers oxygenated blood from the left side of the heart to the rest of the body and returns deoxygenated blood to the right side.
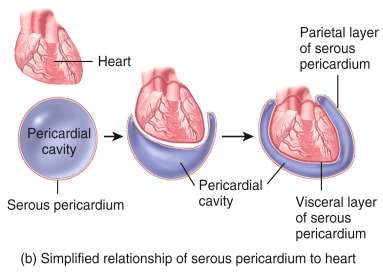
Pericardium and Pericardial Fluid
The heart is enclosed in a double-walled sac called the pericardium, which protects and anchors the heart while allowing it to move during contraction. The pericardium consists of two main layers:
Visceral Pericardium (Epicardium): The inner layer that covers the heart surface.
Parietal Pericardium: The outer layer that forms the pericardial sac.
Pericardial Fluid: A lubricating fluid found between the two layers, reducing friction during heartbeats.
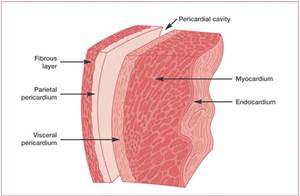
Layers of the Heart Wall
The heart wall is composed of three distinct layers, each with specialized functions:
Epicardium: The outermost layer, also known as the visceral pericardium.
Myocardium: The thick, muscular middle layer responsible for the heart's contractile force.
Endocardium: The smooth, inner lining that reduces friction and lines the heart chambers and valves.
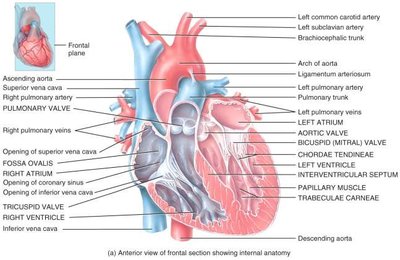
Chambers and Valves of the Heart
The heart contains four chambers and several valves that ensure unidirectional blood flow:
Atria: The two upper, thin-walled chambers that receive blood from the body (right atrium) and lungs (left atrium).
Ventricles: The two lower, thick-walled chambers that pump blood to the lungs (right ventricle) and the body (left ventricle).
Atrioventricular (AV) Valves: The tricuspid (right) and bicuspid/mitral (left) valves separate the atria from the ventricles.
Semilunar Valves: The pulmonary and aortic valves prevent backflow into the ventricles.
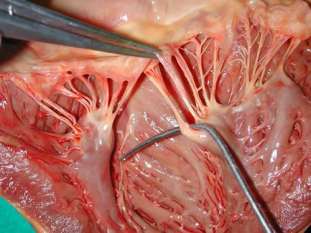
Chordae Tendineae: Tendinous cords that anchor AV valves to papillary muscles, preventing valve prolapse.
Papillary Muscles & Trabeculae Carneae: Muscular projections within the ventricles that support valve function and contraction.
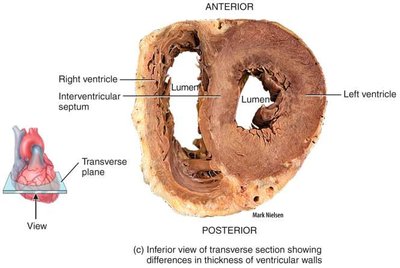
Structural Differences Between Chambers
The left side of the heart is more muscular than the right, reflecting its role in pumping blood throughout the entire body. The left ventricle has a much thicker wall compared to the right ventricle, which only pumps blood to the lungs.
Coronary Circulation
The heart muscle (myocardium) receives its own blood supply through the coronary arteries and veins:
Coronary Arteries: Right and left coronary arteries, marginal, anterior and posterior interventricular, and circumflex arteries supply oxygenated blood to the myocardium.
Coronary Veins: Great, anterior, posterior, middle, and small cardiac veins remove deoxygenated blood and waste, draining into the coronary sinus and then the right atrium.
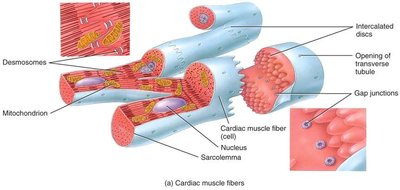
Cardiac Muscle Tissue
Cardiac muscle fibers are specialized for continuous rhythmic contraction and are connected by intercalated discs, which allow rapid transmission of electrical impulses.
Desmosomes: Provide mechanical strength.
Gap Junctions: Allow ions to pass, facilitating synchronized contraction.
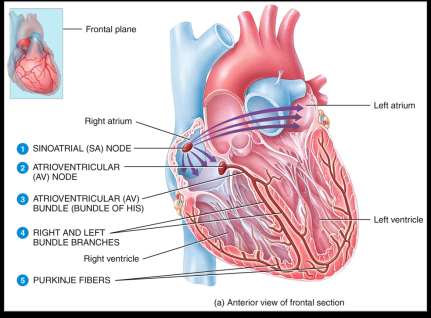
The Cardiac Conduction System
The heart's electrical system coordinates contraction through a specific pathway:
Sinoatrial (SA) Node: The pacemaker; initiates the action potential.
Atrioventricular (AV) Node: Delays the impulse, allowing atrial contraction before ventricular contraction.
AV Bundle (Bundle of His), Bundle Branches, Purkinje Fibers: Distribute the impulse through the ventricles for coordinated contraction.
Electrocardiogram (EKG/ECG)
An EKG records the electrical activity of the heart and is used to diagnose cardiac abnormalities. Key components include:
P wave: Atrial depolarization (contraction).
QRS complex: Ventricular depolarization (contraction).
T wave: Ventricular repolarization (relaxation).

Diagnostic Use of EKG
Large QRS: May indicate an enlarged heart.
Enlarged P wave: Possible atrial enlargement.
Missing/inverted P wave: SA node damage.
Lack of QRS after P wave: Heart block or extrasystole.
Enlarged Q: Myocardial infarction.
The Cardiac Cycle
The cardiac cycle consists of one complete contraction and relaxation of all four heart chambers. It includes four main phases:
Atrial systole (contraction)
Atrial diastole (relaxation)
Ventricular systole (contraction)
Ventricular diastole (relaxation)
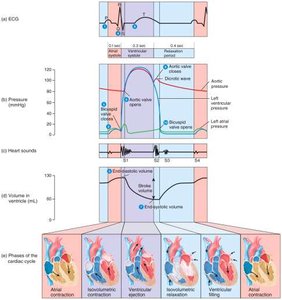
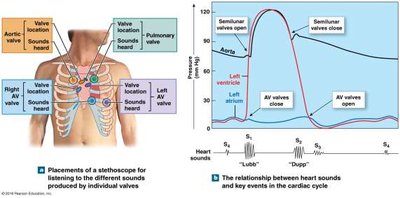
Heart Sounds
Lubb (S1): Closure of AV valves; start of systole.
Dupp (S2): Closure of semilunar valves; start of ventricular diastole.
Heart Murmur: Abnormal sounds due to valve regurgitation.
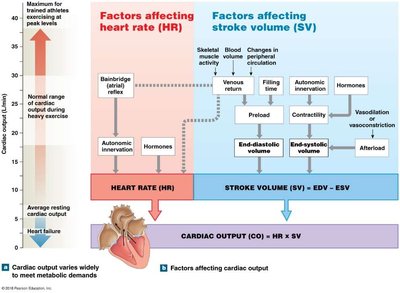
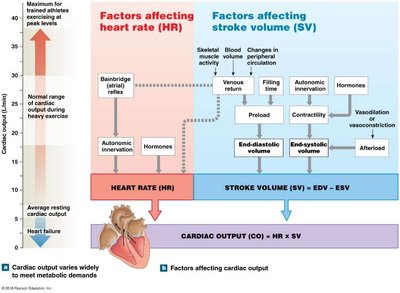
Cardiac Output (CO)
Cardiac output is the volume of blood pumped by each ventricle per minute. It is determined by heart rate (HR) and stroke volume (SV):
Stroke Volume (SV): Amount of blood ejected by a ventricle with each beat.
Heart Rate (HR): Number of heartbeats per minute.
Cardiac Output (CO):
Cardiac Reserve: Difference between resting and maximal cardiac output.
Regulation of Stroke Volume and Heart Rate
Several factors influence stroke volume and heart rate, thereby affecting cardiac output:
Stroke Volume Regulation: Preload (venous return), contractility (strength of contraction), afterload (resistance in arteries).
Heart Rate Regulation: Autonomic nervous system, hormones, venous return.
Summary Table: Factors Affecting Cardiac Output
Factor | Effect on CO |
|---|---|
Heart Rate (HR) | Increased HR increases CO (up to a point) |
Stroke Volume (SV) | Increased SV increases CO |
Preload | Increased preload increases SV and CO |
Contractility | Increased contractility increases SV and CO |
Afterload | Increased afterload decreases SV and CO |
Autonomic NS | Sympathetic stimulation increases HR and CO; parasympathetic decreases HR and CO |
Hormones | Epinephrine, norepinephrine increase HR and contractility |
Additional info: Cardiac output adapts to meet the metabolic demands of the body, increasing during exercise and decreasing during rest or heart failure.
