 Back
BackChapter 22: The Respiratory System – Functional Anatomy and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Overview of the Respiratory System
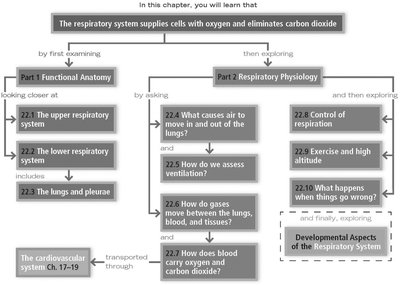
The respiratory system is essential for supplying cells with oxygen and eliminating carbon dioxide. It is divided into two main parts: Functional Anatomy and Respiratory Physiology. This chapter explores the structure, function, and physiological mechanisms of the respiratory system, as well as its developmental aspects and common diseases.
Part 1: Functional Anatomy
22.1 The Upper Respiratory System
The upper respiratory system includes the nose, paranasal sinuses, and pharynx. These structures warm, humidify, and filter incoming air, providing protection and facilitating respiration.
Nose: Provides an airway, moistens and warms air, filters particles, and houses olfactory receptors.
Paranasal Sinuses: Located in the frontal, maxillary, sphenoid, and ethmoid bones; lighten the skull, warm and moisten air, and produce mucus.
Pharynx: Connects the nasal cavity and mouth to the larynx and esophagus; divided into nasopharynx, oropharynx, and laryngopharynx.
Protective Mechanisms: Mucus, lysozyme, defensins, and tonsils trap and destroy pathogens.
22.2 The Lower Respiratory System
The lower respiratory system consists of the larynx, trachea, bronchi, and alveoli. It is divided into conducting and respiratory zones.
Larynx: Routes air and food, produces sound, and prevents aspiration via the epiglottis.
Trachea: Supported by C-shaped cartilage rings; lined with ciliated epithelium to move mucus upward.
Bronchi and Bronchioles: Branch into smaller airways; structural changes occur as airways decrease in size.
Alveoli: Site of gas exchange; type I cells form the respiratory membrane, type II cells secrete surfactant.
22.3 The Lungs and Pleurae
Each lung occupies its own pleural cavity and is divided into lobes and bronchopulmonary segments. The pleurae are double-layered serous membranes that lubricate and protect the lungs.
Lung Structure: Right lung is larger; each lobe has its own blood supply and bronchus.
Pleurae: Parietal pleura lines the thoracic wall; visceral pleura covers the lung surface; pleural fluid reduces friction.
Part 2: Respiratory Physiology
22.4 Pulmonary Ventilation
Volume changes in the thoracic cavity cause pressure changes, leading to air movement. Boyle’s law governs the relationship between pressure and volume.
Intrapulmonary Pressure: Pressure in alveoli; equalizes with atmospheric pressure.
Intrapleural Pressure: Always lower than intrapulmonary pressure, creating a partial vacuum.
Transpulmonary Pressure: Difference between intrapulmonary and intrapleural pressure; determines lung volume.
Physical Factors: Airway resistance, alveolar surface tension (reduced by surfactant), and lung compliance affect ventilation.
22.5 Measuring Respiratory Volumes and Capacities
Respiratory volumes and capacities are measured to assess ventilation and diagnose disorders.
Tidal Volume (TV): Air moved per breath during quiet breathing (~500 ml).
Inspiratory Reserve Volume (IRV): Additional air inhaled after TV (2100–3200 ml).
Expiratory Reserve Volume (ERV): Additional air exhaled after TV (1000–1200 ml).
Residual Volume (RV): Air remaining after maximal exhalation (~1200 ml).
Capacities: Sums of volumes (IC, FRC, VC, TLC).
Anatomical Dead Space: Conducting zone volume (~150 ml) not involved in gas exchange.
Pulmonary Function Tests: Distinguish obstructive (increased TLC, FRC, RV) and restrictive (decreased VC, TLC, FRC, RV) disorders.
22.6 Gas Exchange: Diffusion Between Blood, Lungs, and Tissues
Gases exchange by diffusion, governed by Dalton’s and Henry’s laws.
Dalton’s Law: Total pressure is the sum of partial pressures of each gas.
Henry’s Law: Gas dissolves in liquid in proportion to its partial pressure.
External Respiration: O2 uptake and CO2 unloading; influenced by partial pressure gradients, membrane thickness, and ventilation-perfusion coupling.
Internal Respiration: O2 diffuses into tissues; CO2 diffuses into blood.
22.7 Oxygen and Carbon Dioxide Transport
Oxygen is transported mainly by hemoglobin; carbon dioxide is transported in plasma, on hemoglobin, and as bicarbonate.
Oxygen Transport: 98.5% bound to hemoglobin; affinity affected by temperature, pH, BPG, and CO2 levels.
Carbon Dioxide Transport: 7–10% dissolved, 20% bound to hemoglobin, 70% as bicarbonate.
Hypoxia: Inadequate O2 delivery; classified as anemic, ischemic, histotoxic, hypoxemic, or due to CO poisoning.
22.8 Neural Control of Respiration
Respiratory centers in the brain stem regulate breathing, influenced by chemoreceptors and higher brain centers.
Medulla: VRG (rhythm generation), DRG (integration of sensory input).
Pons: Modifies breathing rhythm, prevents over-inflation.
Chemoreceptors: Respond to CO2, O2, and pH changes.
Higher Centers: Hypothalamus, limbic system, and cortex influence breathing rate and depth.
Reflexes: Pulmonary irritant and inflation reflexes protect airways and lungs.
22.9 Respiratory Adjustments: Exercise and High Altitude
Exercise and altitude affect respiratory function and require physiological adjustments.
Exercise: Hyperpnea increases O2 delivery; hyperventilation leads to low CO2 and alkalosis.
High Altitude: Acclimatization increases ventilation, erythropoietin production, and reduces hemoglobin saturation.
22.10 Respiratory Diseases
Major diseases include COPD, asthma, tuberculosis, and lung cancer.
COPD: Progressive dyspnea, emphysema (enlarged alveoli), chronic bronchitis (excess mucus).
Asthma: Inflammation and constriction of airways.
Tuberculosis: Infectious disease caused by Mycobacterium tuberculosis.
Lung Cancer: Most common malignancy; types include adenocarcinoma, squamous cell carcinoma, and small cell carcinoma.
Developmental Aspects of the Respiratory System
The respiratory system develops from embryonic structures and undergoes changes throughout life.
Embryonic Development: Olfactory placodes form nasal cavities; laryngotracheal bud forms lower respiratory organs.
Fetal Lungs: Filled with fluid; at birth, fluid drains and breathing begins.
Aging: Thoracic wall stiffens, lung elasticity decreases, mucus glands and ciliary action decline.
Key Laws and Equations
Boyle’s Law:
Dalton’s Law:
Henry’s Law: (where C is concentration, k is solubility constant, P is partial pressure)
Carbonic Acid–Bicarbonate Buffer:
Summary Table: Respiratory Volumes and Capacities
Volume/Capacity | Definition | Average Value (ml) |
|---|---|---|
Tidal Volume (TV) | Air moved per breath during quiet breathing | 500 |
Inspiratory Reserve Volume (IRV) | Additional air inhaled after TV | 2100–3200 |
Expiratory Reserve Volume (ERV) | Additional air exhaled after TV | 1000–1200 |
Residual Volume (RV) | Air remaining after maximal exhalation | 1200 |
Vital Capacity (VC) | TV + IRV + ERV | ~4800 |
Total Lung Capacity (TLC) | Sum of all volumes | ~6000 |
Additional info:
Recent discoveries highlight the lungs' role in platelet and blood stem cell production, and the influence of diet and hormones on respiratory health.
Cross-references to other chapters provide context for related anatomical and physiological concepts.
