 Back
BackChapter 22: The Respiratory System – Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Respiratory System Overview
Main Functions and Divisions
The respiratory system is responsible for delivering oxygen to the blood and removing carbon dioxide from the body. It is essential for cellular respiration and maintaining homeostasis. The system is divided both structurally and functionally:
Structurally:
Upper respiratory tract: Nose to larynx
Lower respiratory tract: Trachea to alveoli
Functionally:
Conducting zone: Nose to terminal bronchioles (air passageways only)
Respiratory zone: Respiratory bronchioles and alveoli (sites of gas exchange)
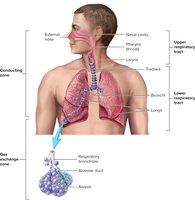
Processes of Respiration
Pulmonary Ventilation and Gas Exchange
Respiration involves two main processes:
Pulmonary ventilation: Movement of air into and out of the lungs.
Gas exchange: Diffusion of gases across cell membranes.
External respiration: Gas exchange between alveolar air and blood.
Internal respiration: Gas exchange between blood and body tissues.
Anatomy of the Respiratory System
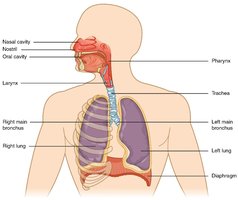
Upper Respiratory Tract
Nasal cavity: Air passageway; cleans, warms, humidifies air; contains olfactory epithelium; resonance for speech.
Pharynx: Passageway between nasal cavity and larynx.
Larynx: Passageway between pharynx and trachea; contains vocal cords for voice production; protected by thyroid and cricoid cartilages; epiglottis prevents food entry during swallowing.
Lower Respiratory Tract
Trachea: Windpipe; reinforced by C-shaped hyaline cartilage rings; splits into primary bronchi.
Bronchi and Bronchioles: Branching airways; smooth muscle regulates diameter (bronchodilation and bronchoconstriction).
Terminal bronchioles: Last part of conducting zone; lined with simple cuboidal epithelium.
Respiratory bronchioles: Beginning of respiratory zone; some alveoli present.
Alveolar ducts and sacs: Passageways and clusters of alveoli; main sites of gas exchange.
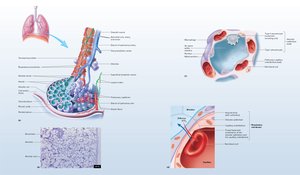
Alveolar Structure and Cells
Type I pneumocytes: Simple squamous cells; form most of alveolar surface; allow efficient gas exchange.
Type II pneumocytes: Cuboidal cells; secrete surfactant to reduce surface tension.
Alveolar macrophages: Patrol and remove debris and pathogens.
The respiratory membrane consists of alveolar and capillary simple squamous epithelium and their fused basement membranes, forming the barrier for gas diffusion.
Mechanics of Breathing
Muscles of Pulmonary Ventilation
Inhalation: Active process; diaphragm contracts and flattens, external intercostals expand rib cage, accessory muscles assist during deep breathing.
Exhalation: Passive at rest (elastic recoil); active during forceful breathing (internal intercostals and abdominal muscles contract).
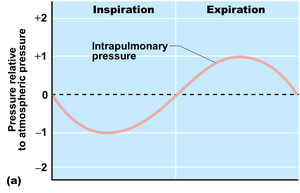
Pressure Gradients and Air Flow
Air moves from areas of higher to lower pressure. During inhalation, thoracic volume increases, intrapulmonary pressure drops below atmospheric pressure, and air enters the lungs. During exhalation, thoracic volume decreases, intrapulmonary pressure rises above atmospheric pressure, and air exits the lungs.
Blood and Lymphatic Supply to the Lungs
Pulmonary arteries: Carry deoxygenated blood to lungs for oxygenation.
Bronchial arteries: Supply oxygenated blood to lung tissues.
Lymphatic vessels: Drain lung tissue and pleura.
Pulmonary Volumes and Capacities
Spirometry and Lung Volumes
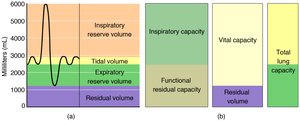
Tidal volume (TV): Air moved per breath during quiet breathing (~500 mL).
Inspiratory reserve volume (IRV): Extra air inhaled after normal inspiration (~3000 mL).
Expiratory reserve volume (ERV): Extra air exhaled after normal expiration (~1100 mL).
Residual volume (RV): Air remaining after maximal exhalation (~1200 mL).
Pulmonary capacities are sums of volumes:
Inspiratory capacity (IC): TV + IRV
Functional residual capacity (FRC): ERV + RV
Vital capacity (VC): IRV + TV + ERV
Total lung capacity (TLC): IRV + TV + ERV + RV
FEV1: Forced Expiratory Volume in 1 second; used to assess lung function in diseases like emphysema.
Other Measurements
Respiratory rate: Breaths per minute.
Minute volume: TV × respiratory rate.
Anatomic dead space: Conducting zone volume where no gas exchange occurs.
Physiological dead space: Anatomic dead space plus poorly ventilated alveoli.
Alveolar ventilation (VA): Volume of air available for gas exchange per minute.
Compliance: Ease of lung and thorax expansion; low compliance means stiff lungs, high compliance means easy expansion but less recoil.
Composition of Inspired, Alveolar, and Expired Air
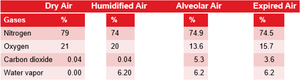
The composition of gases changes as air moves through the respiratory system. Oxygen is highest in outside air and lowest in alveoli due to mixing with residual air and absorption by blood. Exhaled air contains more oxygen than alveolar air due to mixing with air from the conducting zone.
Gases | Dry Air (%) | Humidified Air (%) | Alveolar Air (%) | Expired Air (%) |
|---|---|---|---|---|
Nitrogen | 79 | 74 | 74.9 | 74.5 |
Oxygen | 21 | 20 | 13.6 | 15.7 |
Carbon dioxide | 0.04 | 0.04 | 5.3 | 3.6 |
Water vapor | 0.00 | 6.20 | 6.2 | 6.2 |
Lung Recoil and Pleural Pressure
Lung recoil: Elastic fibers and surface tension in alveoli cause lungs to recoil after stretching.
Surfactant: Reduces surface tension, preventing alveolar collapse.
Pleural membrane: Keeps lungs expanded against thoracic wall; intrapleural pressure is always less than atmospheric pressure.
Pneumothorax: If air enters the pleural space, lung collapses due to loss of negative pressure.
Gas Exchange Mechanisms
External respiration: Oxygen diffuses from alveoli to blood; carbon dioxide diffuses from blood to alveoli.
Internal respiration: Oxygen diffuses from blood to tissues; carbon dioxide diffuses from tissues to blood.
Control of Respiration
Chemoreceptors: Detect changes in blood pH, CO2, and O2 levels.
Primary control: Blood CO2 levels (affecting pH) are the main driver of respiratory rate.
Local control: In lungs, low O2 causes arterioles to constrict, shunting blood to better-ventilated areas.
Respiratory Disorders
Chronic Obstructive Pulmonary Disease (COPD)
Includes chronic bronchitis and emphysema.
Common features:
History of smoking or air pollution exposure
Progressive labored breathing (dyspnea)
Frequent coughing and infections
Hypoxia, CO2 retention, respiratory acidosis, and eventual respiratory failure
Emphysema: Loss of alveolar walls reduces surface area for gas exchange and lung recoil, impairing ventilation.
