 Back
BackChapter 8: Joints (Articulations) – Structure, Function, and Clinical Aspects
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Joints: An Introduction
Joints, or articulations, are anatomical structures where two or more bones meet. They are essential for providing the skeleton with mobility and stability. Understanding joints is crucial for diagnosing and treating musculoskeletal injuries and diseases.
Classification of Joints
Structural Classification
Fibrous Joints: Bones joined by dense fibrous connective tissue; no joint cavity; mostly immovable.
Cartilaginous Joints: Bones united by cartilage; no joint cavity; not highly movable.
Synovial Joints: Bones separated by a fluid-filled joint cavity; freely movable.
Functional Classification
Synarthroses: Immovable joints
Amphiarthroses: Slightly movable joints
Diarthroses: Freely movable joints
Note: Structural classification is most commonly used in anatomical study.
Fibrous Joints
Fibrous joints are connected by dense fibrous connective tissue and lack a joint cavity. Most are immovable, but the degree of movement depends on the length of the connective tissue fibers.
Sutures
Rigid, interlocking joints found only in the skull.
Allow for growth during youth; ossify and fuse in middle age (synostoses).

Syndesmoses
Bones connected by ligaments (bands of fibrous tissue).
Movement varies with fiber length: short fibers (e.g., inferior tibiofibular joint) allow little movement; longer fibers (e.g., interosseous membrane between radius and ulna) allow more movement.

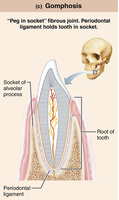
Gomphoses
Peg-in-socket joints (e.g., teeth in alveolar sockets).
Periodontal ligament holds tooth in socket.
Cartilaginous Joints
Cartilaginous joints unite bones with cartilage and lack a joint cavity. They are not highly movable.
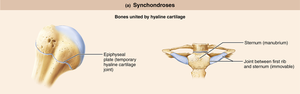
Synchondroses
Bones united by a bar or plate of hyaline cartilage.
Almost all are synarthrotic (immovable).
Examples: epiphyseal plates in children, joint between first rib and manubrium of sternum.
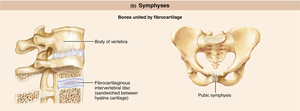
Symphyses
Bones united by fibrocartilage.
Strong, amphiarthrotic (slightly movable) joints.
Examples: intervertebral discs, pubic symphysis.
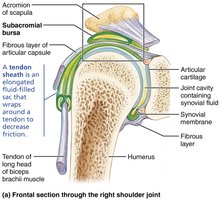
Synovial Joints
Synovial joints are the most common and freely movable joints in the body. They are characterized by a fluid-filled joint cavity.
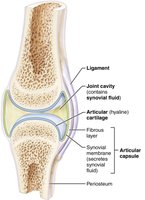
General Structure
Articular cartilage: Hyaline cartilage covering bone ends, preventing crushing of bone ends.
Joint (synovial) cavity: Small, fluid-filled space unique to synovial joints.
Articular (joint) capsule: Two layers—external fibrous layer (dense irregular connective tissue) and inner synovial membrane (loose connective tissue that makes synovial fluid).
Synovial fluid: Viscous, slippery filtrate of plasma and hyaluronic acid; lubricates and nourishes articular cartilage.
Reinforcing ligaments: Capsular, extracapsular, and intracapsular ligaments stabilize the joint.
Nerves and blood vessels: Nerves detect pain and monitor joint position; capillary beds supply filtrate for synovial fluid.
Bursae and Tendon Sheaths
Bursae: Fluid-filled sacs that reduce friction where ligaments, muscles, skin, tendons, or bones rub together.
Tendon sheaths: Elongated bursae that wrap around tendons subjected to friction.

Factors Influencing Stability
Shape of articular surfaces (minor role)
Ligament number and location (limited role)
Muscle tone (most important): Keeps tendons taut as they cross joints, especially important in shoulder and knee joints.
Movements Allowed by Synovial Joints
Gliding Movements
One flat bone surface glides or slips over another similar surface. Examples include intercarpal and intertarsal joints, and between articular processes of vertebrae.

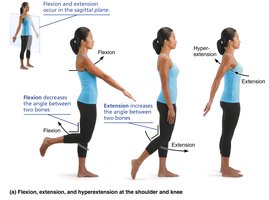
Angular Movements
Flexion: Decreases the angle of the joint.
Extension: Increases the angle of the joint.
Hyperextension: Movement beyond the anatomical position.

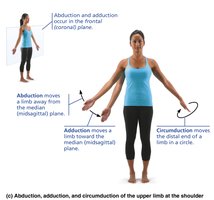
Abduction: Movement away from the midline.
Adduction: Movement toward the midline.
Circumduction: Limb describes a cone in space, involving flexion, abduction, extension, and adduction.
Rotational Movements
Rotation: Turning of a bone around its own long axis (medial or lateral rotation).
Examples: Rotation between vertebrae, rotation of humerus and femur.

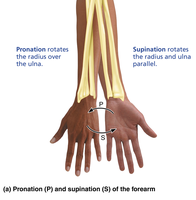
Special Movements
Supination and Pronation: Rotation of the radius and ulna (supination: palms anterior, pronation: palms posterior).
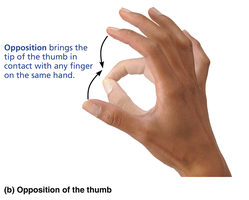
Opposition: Movement of the thumb to touch the tips of other fingers.
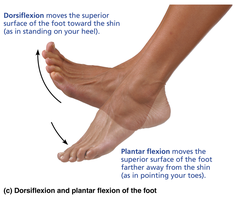
Dorsiflexion and Plantar Flexion: Dorsiflexion bends the foot toward the shin; plantar flexion points the toes.
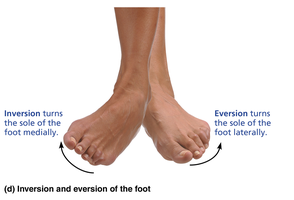
Inversion and Eversion: Inversion turns the sole of the foot medially; eversion turns it laterally.
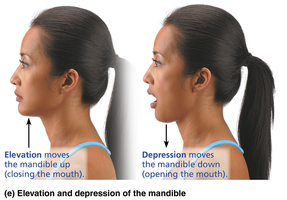
Elevation and Depression: Elevation lifts a body part superiorly (e.g., closing the mouth); depression lowers it (e.g., opening the mouth).
Protraction and Retraction: Protraction moves a body part anteriorly; retraction moves it posteriorly.
Types of Synovial Joints
Synovial joints are classified by the shape of their articular surfaces and the movements they allow:
Plane: Flat articular surfaces; allow gliding movements.
Hinge: Cylindrical projection fits into a trough-shaped surface; allows flexion and extension.
Pivot: Rounded end of one bone fits into a ring; allows rotation.
Condylar (Ellipsoid): Oval articular surface fits into a complementary depression; allows all angular movements.
Saddle: Articular surfaces have both concave and convex areas; allows greater movement than condyloid joints.
Ball-and-Socket: Spherical head of one bone fits into a cup-like socket; allows the most movement (e.g., shoulder, hip).
Clinical Aspects and Disorders of Joints
Common Joint Injuries
Cartilage Tears: Often due to compression and shear stress; may require arthroscopic surgery.
Sprains: Ligaments are stretched or torn; healing is slow due to poor vascularization.
Dislocations (Luxations): Bones forced out of alignment; must be reduced to treat.
Inflammatory and Degenerative Conditions
Bursitis: Inflammation of a bursa, usually from friction or trauma.
Tendonitis: Inflammation of tendon sheaths, typically from overuse.
Arthritis: Over 100 types; most common are osteoarthritis, rheumatoid arthritis, and gouty arthritis.
Osteoarthritis (OA): Degenerative, "wear-and-tear" arthritis; cartilage is broken down faster than it is replaced.
Rheumatoid Arthritis (RA): Chronic, autoimmune disease; immune system attacks joint tissues, leading to deformity.
Gouty Arthritis: Uric acid crystals deposit in joints, causing inflammation; often affects the big toe.
Lyme Disease: Bacterial infection transmitted by ticks; can lead to joint pain and arthritis.
Developmental Aspects of Joints
By embryonic week 8, synovial joints resemble adult joints.
Joint structure is modified by use; active joints have thicker capsules and ligaments.
Aging leads to shortening and weakening of ligaments and tendons; exercise helps maintain joint health.
