 Back
BackComprehensive Study Notes: Anatomy and Physiology of the Heart
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Overview of the Heart
Position, Size, and Shape of the Heart
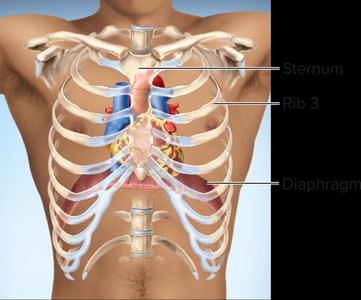
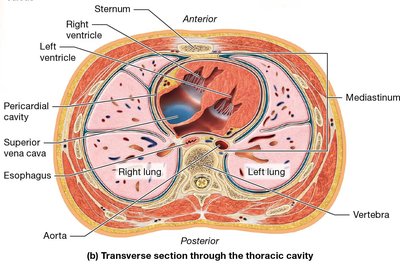
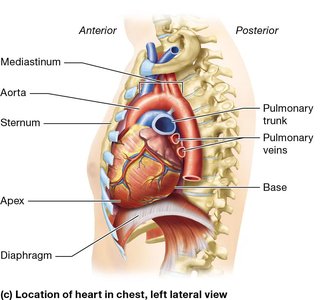
The heart is a muscular organ located in the thoracic cavity, slightly left of the midline, between the lungs. It is roughly the size of a fist and shaped like a cone, with its base directed toward the right shoulder and its apex pointing down and to the left. - Position: The heart sits within the mediastinum, bordered by the lungs, sternum, and diaphragm. - Size: Average adult heart weighs 250-350 grams. - Shape: Cone-shaped, with a broad base and pointed apex. 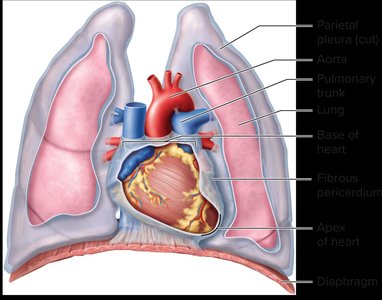
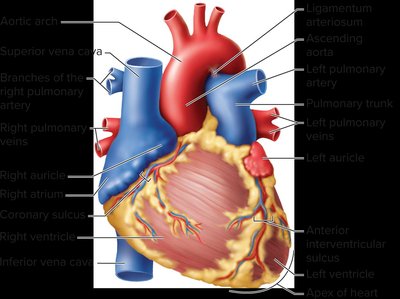
Surface Anatomy of the Heart Chambers
The heart consists of four chambers: two atria (upper chambers) and two ventricles (lower chambers). The surface anatomy is defined by the external grooves (sulci) and the internal septa that separate these chambers. - Right atrium: Receives deoxygenated blood from the body. - Right ventricle: Pumps blood to the lungs. - Left atrium: Receives oxygenated blood from the lungs. - Left ventricle: Pumps blood to the body. 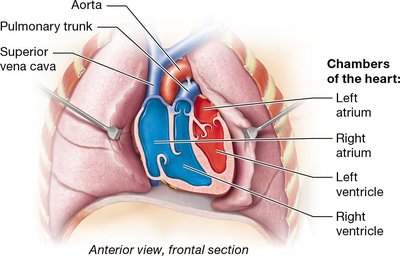
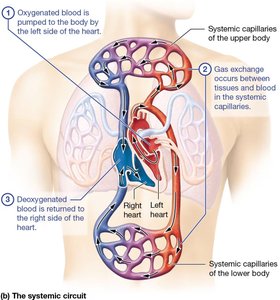
Double Pump Function of the Heart
The heart functions as a double pump, separating pulmonary and systemic circulation. This ensures efficient oxygenation and distribution of blood. - Pulmonary circuit: Right side of the heart pumps deoxygenated blood to the lungs for gas exchange. - Systemic circuit: Left side of the heart pumps oxygenated blood to the rest of the body. 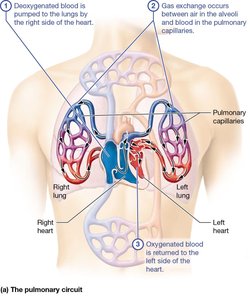
Heart Anatomy and Blood Flow Pathway
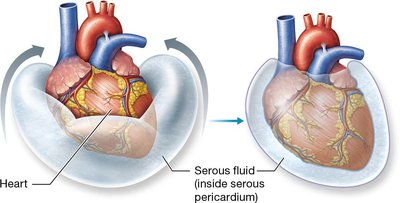
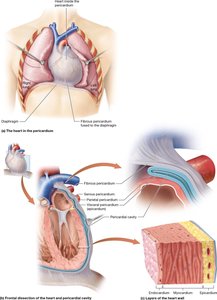
Layers of the Pericardium and Heart Wall
The heart is surrounded by the pericardium, a double-walled sac that protects and anchors the heart. The heart wall itself consists of three layers. - Pericardium: Includes fibrous and serous layers; contains pericardial fluid to reduce friction. - Epicardium: Outer layer, also known as visceral pericardium. - Myocardium: Middle, muscular layer responsible for contraction. - Endocardium: Inner layer lining the heart chambers. 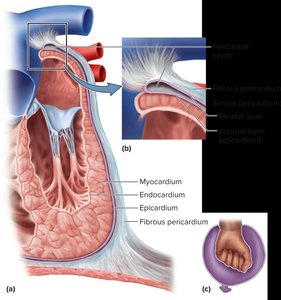
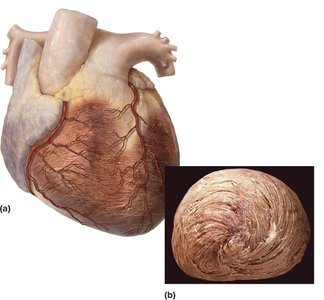
Coronary Circulation and Great Vessels
The coronary circulation supplies blood to the heart muscle itself. Major vessels include the left and right coronary arteries, which branch off the ascending aorta. - Coronary arteries: Deliver oxygen-rich blood to myocardium. - Coronary veins: Drain deoxygenated blood from myocardium into the right atrium via the coronary sinus. 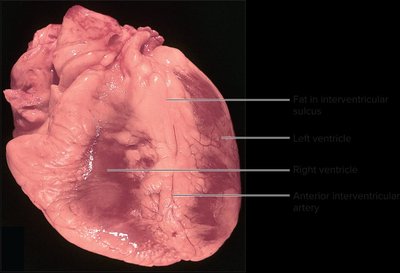
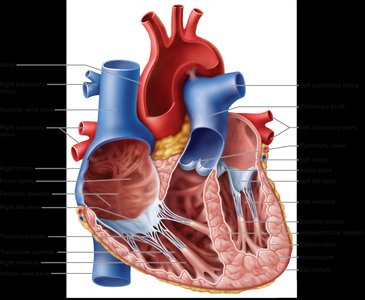
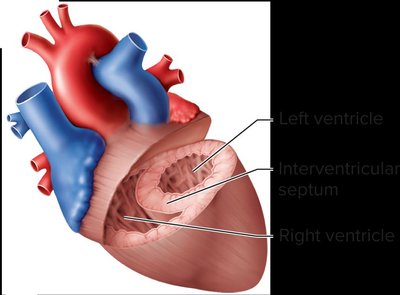
Structure and Function of Chambers, Septa, and Valves
The heart's internal anatomy includes four chambers, separated by septa and regulated by valves to ensure unidirectional blood flow. - Interatrial septum: Separates right and left atria. - Interventricular septum: Separates right and left ventricles. - Valves: Prevent backflow; include atrioventricular (tricuspid and mitral) and semilunar (aortic and pulmonary) valves. 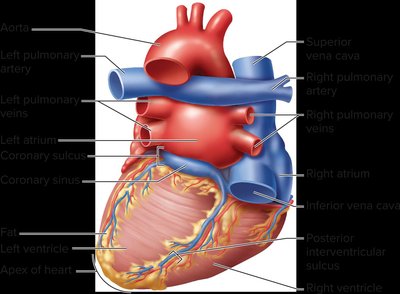
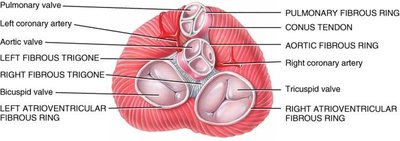
Cardiac Skeleton
The cardiac skeleton is a plate of fibrous connective tissue that provides structural support and electrical insulation between the atria and ventricles. - Fibrous rings: Surround heart valves, supporting their function. - Electrical insulation: Prevents direct conduction between atria and ventricles. 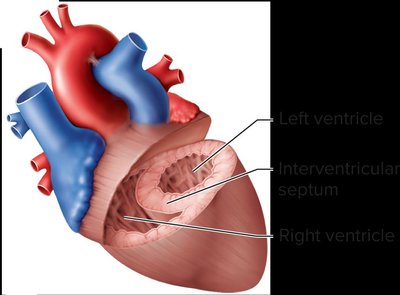
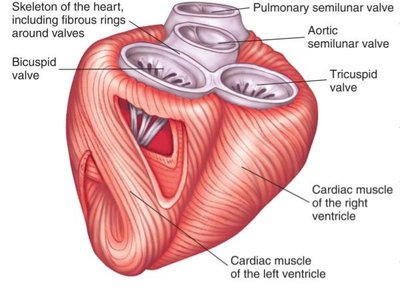
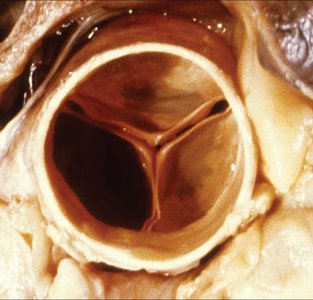
Valves of the Heart
The heart contains four main valves: tricuspid, mitral (bicuspid), aortic, and pulmonary. These valves ensure blood flows in one direction. - Atrioventricular valves: Tricuspid (right), mitral (left). - Semilunar valves: Aortic and pulmonary. - Chordae tendineae and papillary muscles: Prevent valve prolapse during contraction. 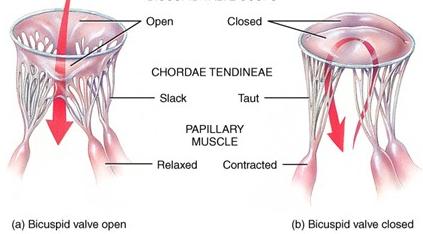
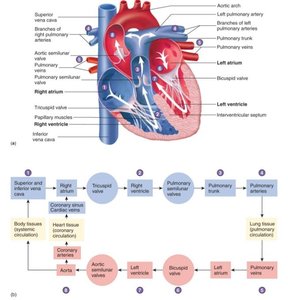
Pathway of Blood Flow Through the Heart
Blood flows through the heart in a specific sequence, regulated by valves and pressure gradients.
Step | Chamber/Valve | Direction |
|---|---|---|
1 | Right atrium | Receives deoxygenated blood from body |
2 | Tricuspid valve | To right ventricle |
3 | Right ventricle | Pumps blood to lungs via pulmonary valve |
4 | Left atrium | Receives oxygenated blood from lungs |
5 | Mitral valve | To left ventricle |
6 | Left ventricle | Pumps blood to body via aortic valve |
Coronary Circulation
The coronary arteries supply oxygenated blood to the myocardium, while coronary veins return deoxygenated blood to the right atrium. - Left main coronary artery: Branches into left anterior descending and circumflex arteries. - Venous drainage: Via great cardiac vein, middle cardiac vein, left marginal vein, and coronary sinus.
Cardiac Muscle Tissue Anatomy and Electrophysiology
Histology of Cardiac Muscle Tissue
Cardiac muscle cells (cardiomyocytes) are elongated, branching cells with 1-2 centrally located nuclei. They are connected by intercalated disks, which contain desmosomes and gap junctions. - Intercalated disks: Specialized cell-cell contacts for mechanical and electrical connectivity. - Desmosomes: Hold cells together. - Gap junctions: Allow action potentials to pass rapidly between cells.
Cardiac Muscle Gated Ion Channels
Cardiac muscle cells contain several types of ion channels in their sarcolemma, which are essential for action potential generation and propagation. - Voltage-gated sodium channels - Voltage-gated calcium channels (with time-gated closing) - Potassium channels (ligand-gated and voltage-gated) - Nonselective cation channels (activated by hyperpolarization)
Cardiac Pacemaker Action Potential
The sinoatrial (SA) node generates spontaneous action potentials, leading to the heart's autorhythmicity. - Phases: Rapid depolarization (Na+ influx), plateau (Ca2+ influx), repolarization (K+ efflux). - Importance: Plateau phase prevents tetanic contractions, ensuring rhythmic heartbeats.
Cardiac Conduction System
The cardiac conduction system coordinates the heartbeat, ensuring efficient contraction. - Sinoatrial (SA) node: Primary pacemaker. - Atrioventricular (AV) node: Delays impulse. - Bundle of His, bundle branches, Purkinje fibers: Distribute impulse to ventricles.
Electrocardiogram (ECG) Waveforms
The ECG records electrical activity of the heart. - P wave: Atrial depolarization. - QRS complex: Ventricular depolarization (and atrial repolarization). - T wave: Ventricular repolarization. - PR interval: Time from atrial to ventricular contraction. - QT interval: Duration of ventricular contraction and relaxation.
Mechanical Physiology of the Heart: The Cardiac Cycle
Phases of the Cardiac Cycle
The cardiac cycle consists of systole (contraction) and diastole (relaxation) of the heart chambers. - Systole: Ejection of blood from chambers. - Diastole: Filling of chambers. - Cycle: One complete contraction and relaxation of all four chambers.
Pressure and Volume Changes
Pressure changes in the heart govern the opening and closing of valves, ensuring unidirectional blood flow. - Left ventricle: Pressure rises during contraction, forcing blood into the aorta. - Mitral valve: Opens during relaxation, allowing blood to flow into ventricle.
Heart Sounds
Heart sounds are produced by the closing of valves. - First sound ("lubb"): AV valves close at beginning of ventricular systole. - Second sound ("dubb"): Semilunar valves close at beginning of ventricular diastole. - Third sound: Occasional, due to turbulent blood flow during diastole.
Heart Murmurs
Murmurs are abnormal heart sounds caused by turbulent blood flow, often due to valve stenosis or regurgitation. - Valve stenosis: Narrowed valve opening. - Valve regurgitation: Incomplete valve closure.
Cardiac Output and Regulation
Definition and Calculation of Cardiac Output
Cardiac output (CO) is the volume of blood pumped by either ventricle per minute. It is determined by stroke volume (SV) and heart rate (HR). - Formula: - Stroke volume: (End-diastolic volume minus end-systolic volume) - Ejection fraction: Percentage of blood ejected per beat; normal EF is 55-70%.
Factors Influencing Cardiac Output
- Preload: Degree of stretch of ventricular walls; governed by Frank-Starling law. - Contractility: Force of myocardial contraction for a given preload. - Afterload: Pressure ventricles must overcome to eject blood.
Frank-Starling Law
The greater the stretch of ventricular muscle cells, the more forcefully they contract, increasing stroke volume.
Extrinsic Regulation: Autonomic Nervous System
Neural and hormonal control modulates heart rate and contractility. - Parasympathetic stimulation: Decreases heart rate via vagus nerve and acetylcholine. - Sympathetic stimulation: Increases heart rate and contractility via norepinephrine and epinephrine. - Hormonal control: Epinephrine and norepinephrine from adrenal medulla.
Central Nervous System and the Heart
- Proprioceptors: In muscles and joints, signal increased metabolic demand. - Baroreceptors: Pressure sensors in aorta and carotid arteries, regulate blood pressure and heart rate. - Chemoreceptors: Sensitive to blood pH, CO2, and O2 levels.
Pathology: Myocardial Infarction and Heart Failure
Myocardial Infarction (MI)
MI is the death of myocardium due to interruption of blood flow, commonly caused by atherosclerosis and thrombosis. - Symptoms: Angina pectoris, chest pain, elevated troponin levels.
Congestive Heart Failure (CHF)
CHF results from the failure of either ventricle to eject blood effectively, leading to pulmonary or systemic edema. - Left ventricular failure: Pulmonary edema, shortness of breath. - Right ventricular failure: Systemic edema, liver enlargement, extremity swelling.
Cardiomyopathy
Types include hypertrophic, dilated, restrictive, and congestive cardiomyopathy. - Dilated cardiomyopathy: Thinned, weakened heart wall. - Hypertrophic cardiomyopathy: Thickened heart wall.
Summary Table: Cardiac Output Regulation
Factor | Effect on Cardiac Output |
|---|---|
Preload | Increases stroke volume via Frank-Starling law |
Contractility | Increases stroke volume |
Afterload | Decreases stroke volume if increased |
Heart Rate | Increases cardiac output if increased |
Parasympathetic stimulation | Decreases heart rate and cardiac output |
Sympathetic stimulation | Increases heart rate and cardiac output |
Key Equations
Cardiac Output: Stroke Volume: Ejection Fraction: Frank-Starling Law: Force of contraction increases with increased muscle stretch (preload).
Additional info:
Some details, such as the precise values for normal ejection fraction and the mechanisms of baroreceptor and chemoreceptor reflexes, were inferred from standard academic sources to ensure completeness and clarity.
