 Back
BackComprehensive Study Notes: Cardiac Anatomy, Physiology, and Electrocardiography (Chapters 1–6)
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Cardiac Anatomy and Physiology
Layers of the Heart
The heart is composed of three distinct layers, each with specialized functions essential for cardiac performance and protection.
Epicardium: The outermost layer, housing the coronary arteries that supply blood to the heart muscle.
Myocardium: The thick, muscular middle layer responsible for contraction and pumping blood. This layer is most affected during a heart attack.
Endocardium: The innermost, watertight layer lining the chambers and forming the heart valves. It contains the conduction system that regulates heartbeat.
Function: These layers work together to ensure efficient blood flow and structural integrity of the heart.
Heart Chambers and Oxygenation Status
The heart contains four chambers, each with a specific role in blood circulation and oxygenation:
Right Atrium: Receives deoxygenated blood from the body (60–75% oxygen saturation; dark maroon).
Right Ventricle: Pumps deoxygenated blood to the lungs for oxygenation (similar saturation as right atrium).
Left Atrium: Receives oxygenated blood from the lungs (~100% oxygen saturation; bright red).
Left Ventricle: Pumps oxygenated blood throughout the body (~100% oxygen saturation; bright red).
Heart Valves
Valves ensure unidirectional blood flow and prevent backflow:
Atrioventricular (AV) Valves:
Tricuspid Valve: Between right atrium and right ventricle (three cusps).
Mitral (Bicuspid) Valve: Between left atrium and left ventricle (two cusps).
Semilunar Valves:
Pulmonic Valve: Between right ventricle and pulmonary artery.
Aortic Valve: Between left ventricle and aorta.
Mechanism: Valves open and close in response to pressure changes, ensuring blood flows in the correct direction.
Great Vessels of the Heart
Superior Vena Cava (SVC): Returns deoxygenated blood from the upper body to the right atrium.
Inferior Vena Cava (IVC): Returns deoxygenated blood from the lower body to the right atrium.
Pulmonary Artery: Carries deoxygenated blood from the right ventricle to the lungs.
Pulmonary Veins: Carry oxygenated blood from the lungs to the left atrium.
Aorta: Distributes oxygenated blood from the left ventricle to the body.
Blood Flow Through the Heart
Systemic Circulation: Aorta → arteries → arterioles → capillaries (oxygen delivered) → venules → veins → vena cava (deoxygenated blood returns).
Cardiac Circulation: Coronary arteries supply the myocardium; deoxygenated blood returns via coronary veins to the right atrium.
The Cardiac Cycle
Diastole (Ventricular Relaxation): Rapid-filling phase, diastasis, atrial kick.
Systole (Ventricular Contraction): Isovolumetric contraction, ventricular ejection, protodiastole, isovolumetric relaxation.
Coronary Arteries
Left Anterior Descending (LAD): Supplies anterior left ventricle and septum.
Circumflex Artery: Supplies left atrium and lateral/posterior left ventricle.
Right Coronary Artery (RCA): Supplies right atrium, right ventricle, and often inferior left ventricle.
Types of Cardiac Cells
Contractile Cells: Responsible for heart muscle contraction.
Conduction System Cells: Generate and conduct electrical impulses.
Nervous Control of the Heart
Sympathetic Nervous System: Increases heart rate and contractility (fight-or-flight response).
Parasympathetic Nervous System: Decreases heart rate (rest-and-digest state).
Electrophysiology
Polarization, Depolarization, and Repolarization
Polarized: Resting state; inside of cell is negatively charged.
Depolarization: Sodium influx makes inside positive; triggers contraction.
Repolarization: Potassium efflux restores negative charge; triggers relaxation.
Action Potential Phases
Phase 4: Resting (polarized, -90 mV).
Phase 0: Depolarization (Na+ influx, positive inside).
Phase 1: Early repolarization (K+ efflux).
Phase 2: Plateau (Ca2+ influx balances K+ efflux).
Phase 3: Rapid repolarization (K+ efflux, return to negative).
Refractory Periods
Absolute: No new action potential possible.
Relative: Strong stimulus can trigger action potential.
Supernormal: Weaker-than-normal stimulus can trigger action potential.
EKG Waves and Segments
P Wave: Atrial depolarization.
QRS Complex: Ventricular depolarization.
T Wave: Ventricular repolarization.
PR Segment: End of P wave to start of QRS; AV node conduction.
ST Segment: End of QRS to start of T wave; ventricular contraction.
Labeling a Rhythm Strip
P wave, PR segment, PR interval, QRS complex (Q, R, S waves), ST segment, T wave, QT interval.
Heart Walls and Corresponding Leads
Anterior: V2–V4
Lateral: I, aVL, V5, V6
Inferior: II, III, aVF
Septal: V1, V2
Posterior: V7–V9 (or reciprocal changes in V1–V3)
EKG Paper Measurements
Small box: 0.04 sec (time), 0.1 mV (amplitude)
Large box: 0.20 sec (time), 0.5 mV (amplitude)
Electrocardiography: Lead Morphology and Placement
Electrodes and Leads
Electrode: Sensor placed on skin to detect electrical signals.
Lead: A specific view of the heart’s electrical activity, created by measuring voltage differences between electrodes.
Bipolar and Unipolar Leads
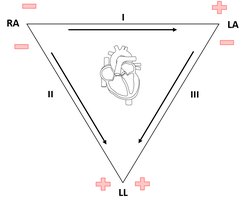
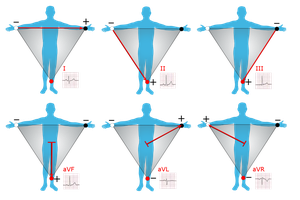
Bipolar Leads: I (RA–LA), II (RA–LL), III (LA–LL); measure between two points.
Unipolar Augmented Leads: aVR (right arm), aVL (left arm), aVF (left leg); use a single positive electrode and a reference point.
Einthoven’s Law and Triangle
Einthoven’s Law: Lead II = Lead I + Lead III
Einthoven’s Triangle: Visualizes the relationship between limb electrodes and bipolar leads.
Precordial (Chest) Leads
V1: 4th intercostal space, right sternal border
V2: 4th intercostal space, left sternal border
V3: Between V2 and V4
V4: 5th intercostal space, midclavicular line
V5: Level with V4, anterior axillary line
V6: Level with V4, midaxillary line
Continuous Monitoring Leads
Lead II and V1/MCL1 are most commonly used for continuous monitoring in hospitals.
Electrocardiographic Truths
Impulse toward positive electrode: upward (positive) QRS
Impulse away from positive electrode: downward (negative) QRS
Impulse perpendicular: isoelectric complex
Normal QRS Complex Deflections in 12-Lead EKG
Leads I, II, III, aVL, aVF: Positive QRS
aVR: Negative QRS
V1, V2: Negative QRS
V3, V4: Isoelectric (transition zone)
V5, V6: Positive QRS
Technical Aspects of the EKG
Control Features of an EKG Machine
Chart Speed: Standard is 25 mm/sec; affects horizontal (time) scale.
Gain: Standard is 10 mm/mV; affects vertical (voltage) scale.
Frequency Response: Filters out noise/artifact.
Macroshock vs. Microshock
Macroshock: High-voltage shock from faulty equipment; can cause burns or arrhythmias.
Microshock: Low-voltage shock, dangerous for patients with internal devices (e.g., pacemakers).
EKG Artifacts and Troubleshooting
Somatic Tremors: Jittery, erratic baseline from muscle movement.
Baseline Sway: Wandering baseline from breathing or poor electrode contact.
60-Cycle Interference: Thick, fuzzy baseline from electrical devices.
Broken Recording: Abrupt breaks or flat lines from loose/disconnected wires.
Troubleshooting: Check patient movement, electrode placement, wire connections, and minimize electrical interference.
Differentiating Artifact from Real Rhythm
Artifacts are inconsistent, irregular, and often linked to external factors.
Real rhythms are regular, repeatable, and physiologically plausible.
Check multiple leads and observe the patient to confirm findings.
Calculating Heart Rate
Heart Rate Definition
Heart rate is the number of QRS complexes per minute (beats per minute, bpm).
Methods to Calculate Heart Rate
Six-Second Strip Method: Count QRS complexes in 6 seconds, multiply by 10.
Memory (300) Method: 300, 150, 100, 75, 60, 50, 43, 37, 33, 30 (large boxes between QRS).
1500 (Little Block) Method: 1500 divided by number of small boxes between QRS complexes.
Types of Rhythm Regularity
Regular Rhythm: Consistent R-R intervals.
Regular but Interrupted: Premature beats or pauses.
Irregular Rhythm: Unpredictable R-R intervals.
Choosing Calculation Method by Rhythm Regularity
Regular: Use 300 or 1500 method.
Irregular: Use six-second strip method for mean rate.
Interrupted: Use regular portions for calculation; six-second strip for frequent pauses.
How to Interpret a Rhythm Strip
Steps to Rhythm Identification
Check for QRS complexes.
Determine regularity (R-R intervals).
Calculate heart rate.
Identify and describe P waves.
Measure PR interval (0.12–0.20 sec).
Measure QRS complex (<0.12 sec).
Criteria for Normal Sinus Rhythm (NSR)
Regular rhythm (R-R intervals consistent).
Heart rate: 60–100 bpm.
P wave before every QRS; QRS after every P wave.
PR interval: 0.12–0.20 sec.
QRS complex: <0.12 sec.
QT interval: 0.36–0.40 sec (varies with rate).
Arrhythmia
Any rhythm not meeting NSR criteria (except for rate alone).
Caused by conduction system abnormalities or ectopic activity.
May be benign or life-threatening depending on type and context.
Pacemakers of the Heart and Their Inherent Rates
Pacemaker | Location | Inherent Rate (bpm) |
|---|---|---|
Sinoatrial (SA) Node | Right atrium | 60–100 |
Atrioventricular (AV) Node | AV junction | 40–60 |
Purkinje Fibers (Ventricular) | Ventricular walls | 20–40 |
Cardiac Impulse Conduction Pathway
SA node → atrial conducting fibers → AV node → bundle of His → right & left bundle branches → Purkinje fibers
Characteristics of Cardiac Cells
Automaticity: Ability to generate impulses independently.
Conductivity: Ability to transmit impulses to neighboring cells.
Excitability: Ability to respond to electrical stimuli.
Contractility: Ability to contract in response to stimulation.
Escape vs. Usurpation
Escape: Lower pacemaker takes over when higher pacemaker fails (slower rhythm).
Usurpation: Lower pacemaker overrides higher pacemaker by firing faster (faster rhythm).
What Happens When Pacemakers Fail
SA node fails: AV node takes over (40–60 bpm).
SA & AV nodes fail: Purkinje fibers take over (20–40 bpm).
Difference Between Rhythm Strip and 12-Lead EKG
Rhythm Strip: Single lead, continuous monitoring, focuses on rhythm and rate.
12-Lead EKG: Multiple leads, diagnostic, provides comprehensive view of heart’s electrical activity.
