Back
BackDermatologic Disorders: Anatomy, Physiology, and Pathophysiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Dermatology Anatomy and Physiology
Skin Structures
The skin is the largest organ of the body and consists of multiple layers and specialized structures that contribute to its protective, sensory, and regulatory functions.
Epidermis: Outermost layer, composed primarily of keratinocytes.
Dermis: Middle layer, rich in collagen, blood vessels, nerves, and immune cells.
Subcutaneous tissue: Deepest layer, mainly adipose tissue for insulation and energy storage.
Skin appendages: Hair follicles, sebaceous glands, sweat glands, and nails.

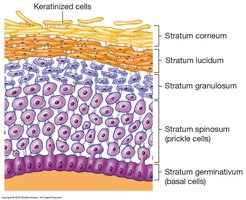
Epidermis: Keratinocytes
Keratinocytes make up about 85% of the epidermis and are responsible for producing keratin, a protein that provides structural strength and protection.
Basal cells: Divide to form new keratinocytes.
Migration: Keratinocytes move upward, changing morphology as they progress through the layers.
Stratum corneum: Outermost, thickest layer; composed of dead, keratinized cells.
Turnover time: 20–30 days for keratinocytes to migrate from the basal layer to the surface.
Epidermis: Melanocytes
Melanocytes are specialized cells located in the basal layer of the epidermis. They produce melanin, the pigment responsible for skin color and protection against ultraviolet (UV) radiation.
Melanosomes: Organelles that package melanin; size determines skin color (larger in darker skin).
Function: Absorb and scatter UV rays to protect underlying tissues.
Conditions: Albinism (lack of melanin), vitiligo (loss of melanocytes), and increased melanin production with UV exposure.
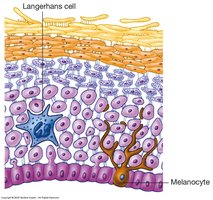
Epidermis: Langerhans Cells
Langerhans cells are dendritic antigen-presenting cells found in the epidermis. They play a crucial role in the skin's immune defense.
Function: Bind antigens, migrate to lymph nodes, and stimulate T-cell proliferation and cytokine release.
Role: Initiate immune responses to pathogens and allergens.

Dermis
The dermis is a collagen-rich layer that provides structural support, nourishment, and immune protection to the skin.
Components: Collagen fibers, blood vessels, nerves, fibroblasts, macrophages, mast cells, and T-cells.
Functions: Nutrient supply, immune surveillance, sensation, and thermoregulation.
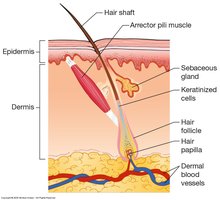
Dermal Appendages
Skin appendages are specialized structures derived from the epidermis but located in the dermis.
Hair follicles: Produce hair; color determined by melanosomes.
Sebaceous glands: Secrete sebum (lipids) to lubricate skin and hair, prevent moisture loss.
Sweat glands: Eccrine (thermoregulation) and apocrine (scent); regulate body temperature.
Nails: Protect distal phalanges and aid in fine manipulation.
Functions of the Skin
The skin serves multiple essential functions for homeostasis and protection.
Temperature regulation: Vasodilation/vasoconstriction and sweat production controlled by the sympathetic nervous system.
Sensory perception: Detects pain, temperature, and touch.
Hydration maintenance: Prevents excessive water loss.
Immunologic barrier: Physical and cellular defense against pathogens.
Hormone synthesis: Converts 7-dehydrocholesterol to cholecalciferol (vitamin D3) upon UV exposure.
Psoriasis
Overview and Epidemiology
Psoriasis is a chronic, immune-mediated skin disorder characterized by periods of remission and exacerbation. It affects approximately 2% of the population, with a bimodal age of onset (20–40 years and 50–60 years).
Genetics: Strong familial association; 60–90% have a family history.
Clinical course: Managed but not cured; relapses are common.
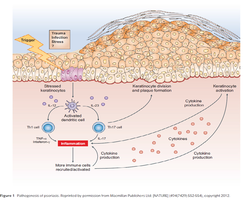
Pathophysiology
Psoriasis involves immune dysregulation, leading to inflammation and abnormal keratinocyte proliferation.
Key immune cells: Th1 and Th17 T-lymphocytes.
Cytokines: IL-22, among others, drive keratinocyte proliferation and poor differentiation.
Keratinocyte transit time: Shortened from 13 to 2 days, resulting in thickened, scaly plaques.
Angiogenesis: Increased blood vessel formation and vasodilation in affected skin.
Etiology and Risk Factors
Trauma: Koebner phenomenon (lesion formation at sites of injury).
Infection: Streptococcal and viral infections (especially in guttate psoriasis).
Lifestyle: Stress, smoking, obesity, alcohol.
Drugs: Lithium, beta blockers, TNF antagonists, hydroxychloroquine, terbinafine, corticosteroid withdrawal.
Types of Psoriasis
Plaque psoriasis (psoriasis vulgaris): Most common (90%).
Other variants: Flexural/intertriginous, erythrodermic, localized (scalp, palms/soles), guttate, generalized pustular, seborrheic.
Clinical Presentation
Dermatologic features: Pruritus, scaling, erythema, pain, Auspitz phenomenon (bleeding with mild disruption).
Distribution: Commonly elbows, knees, scalp; can be localized or generalized.
Nail involvement: Psoriatic onychodystrophy (pitting, hyperkeratosis, onycholysis, oil-drop discoloration).
Severity: Mild (<5% BSA), moderate (5–10% BSA), severe (>10% BSA or PASI ≥ 10).


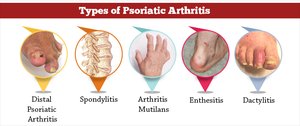
Systemic Manifestations
Psoriatic arthritis: May develop years after skin disease; can involve distal interphalangeal joints, spine, and other sites.
Other comorbidities: Mental health disorders, metabolic syndrome, increased risk of diabetes, cardiovascular disease, Crohn’s disease, and certain malignancies.
Treatment Options
Topical agents: Corticosteroids, vitamin D analogs, keratolytics.
Biologic response modifiers: TNF inhibitors (etanercept, adalimumab, infliximab), IL-17 inhibitors (secukinumab, ixekizumab, brodalumab), IL-12/23 inhibitors (ustekinumab), IL-23 inhibitors (guselkumab).
Atopic Dermatitis (Eczema)
Overview and Epidemiology
Atopic dermatitis is a chronic, inflammatory skin disorder often associated with other atopic conditions such as asthma and allergic rhinitis. Most cases present in early childhood.
Key features: Pruritus (itching), dry skin, and eczematous lesions.
Onset: 60% by age 1, most by age 5.
Pathophysiology
Atopic dermatitis results from a combination of skin barrier dysfunction, immune dysregulation, and microbial imbalance.
Skin barrier disruption: Increased water loss, decreased lipids, increased permeability.
Genetic factors: Filaggrin mutations reduce keratin crosslinking and increase pH.
Microbial dysbiosis: Reduced microbial diversity, predominance of Staphylococcus aureus.
Immune dysfunction: Th2 cytokine activity, increased IgE, and interleukins (IL-4, IL-31) drive inflammation and pruritus.


Clinical Presentation
Infants/children: Weeping vesicles, pruritus, crusting, erythema (often starts on face, spares nose tip).
Adolescents/adults: Dry, red patches, chronic lichenified (thickened) skin, commonly on knees, elbows, neck, hands.



Treatment
Skin moisturization: Emollients to restore barrier function.
Topical corticosteroids: Reduce inflammation.
Topical calcineurin inhibitors: Tacrolimus, pimecrolimus for steroid-sparing effect.
Biologic therapy: Dupilumab (IL-4 receptor antagonist).
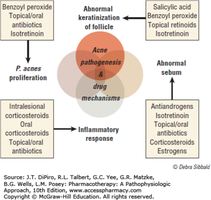
Acne Vulgaris
Overview and Pathogenesis
Acne vulgaris is an inflammatory disorder of the pilosebaceous unit, involving hair follicles and sebaceous glands. It is most common on the face, back, and chest.
Sebum: Lipid-rich secretion produced by sebaceous glands; increased by androgens.
Distribution: Absent on palms and soles; most numerous on face, back, chest.
Acne Terminology
Non-inflammatory lesions: Comedones (dilated hair follicles)
Open comedones: Blackheads (melanin-containing sebum plugs)
Closed comedones: Whiteheads (pale, raised papules)
Inflammatory lesions:
Papules: Raised lesions < 5 mm
Pustules: Central core of pus
Nodules: > 5 mm; may form cysts



Precipitating Factors
Hormones: Androgens increase sebaceous gland size and activity.
Other factors: Heat, humidity, friction, stress, occlusion (cosmetics), diet (dairy, high sugar).
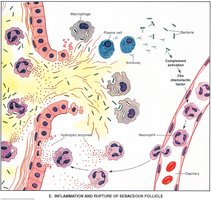
Pathophysiology
Increased sebum production: Androgen-induced.
Colonization by Cutibacterium acnes: Bacterial proliferation in follicles.
Neutrophil infiltration: Inflammatory response to bacterial lipases and follicular rupture.
Follicular hyperkeratinization: Plugged follicles due to increased keratinocyte proliferation.

Treatment
Topical agents: Benzoyl peroxide, retinoids, antibiotics, salicylic acid.
Systemic agents: Oral antibiotics, hormonal therapy, isotretinoin for severe cases.
Mechanisms: Target abnormal keratinization, sebum production, bacterial proliferation, and inflammation.