 Back
BackDigestive System: Pharynx, Esophagus, Stomach, Liver, Gallbladder, and Pancreas
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Pharynx and Esophagus
The Pharynx
The pharynx serves as a passageway for food, fluids, and air, connecting the mouth to the esophagus and larynx. It is lined with stratified squamous epithelium and contains mucus-producing glands for protection and lubrication. The muscular wall consists of an inner longitudinal layer and an outer circular layer of skeletal muscle, which facilitate the movement of food toward the esophagus.
The Esophagus
The esophagus is a flat, muscular tube that connects the laryngopharynx to the stomach. It remains collapsed when not in use and passes through the diaphragm at the esophageal hiatus. The gastroesophageal (cardiac) sphincter surrounds the cardial orifice, preventing acid reflux by keeping the orifice closed when food is not being swallowed. Mucus cells on both sides of the sphincter protect the esophagus from stomach acid.
Layers of the Esophagus: mucosa (stratified squamous epithelium), submucosa (with mucus glands), muscularis externa (skeletal muscle superiorly, mixed in the middle, smooth muscle inferiorly), and adventitia (fibrous connective tissue).
The mucosa transitions to simple columnar epithelium at the stomach.


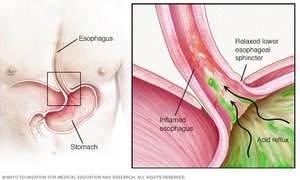
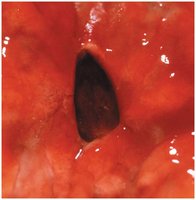
Clinical – Homeostatic Imbalance: Heartburn
Heartburn is caused by the regurgitation of stomach acid into the esophagus, often due to a relaxed lower esophageal sphincter. It is a primary symptom of gastroesophageal reflux disease (GERD) and can be triggered by overeating, obesity, pregnancy, or hiatal hernia. Chronic exposure can lead to esophagitis, ulcers, or esophageal cancer.
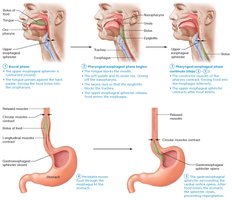
Digestive Processes of the Mouth, Pharynx, and Esophagus
The main function of the pharynx and esophagus is propulsion—moving food from the mouth to the stomach. This process, called deglutition (swallowing), involves the coordinated action of 22 muscle groups and occurs in two phases:
Buccal phase: Voluntary contraction of the tongue to push the bolus into the oropharynx.
Pharyngeal-esophageal phase: Involuntary phase controlled by the vagus nerve and the swallowing center in the medulla and lower pons.
The Stomach
Gross Anatomy of the Stomach
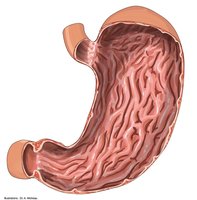
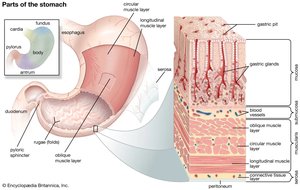
The stomach is a muscular, expandable organ that serves as a temporary storage tank and initiates the chemical breakdown of proteins. It converts food into a semi-liquid mixture called chyme. The stomach can expand from about 50 mL when empty to up to 4 liters after a meal. When empty, its mucosa forms folds called rugae.
Regions of the stomach: cardia, fundus, body, and pyloric part (antrum, canal, pylorus).
The pyloric sphincter controls the passage of chyme into the duodenum.
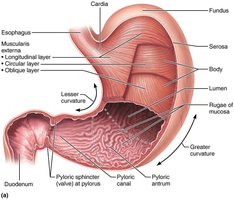

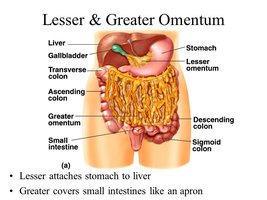
Stomach Curvatures and Mesenteries
The greater curvature is the convex lateral surface, and the lesser curvature is the concave medial surface. The lesser omentum attaches the stomach to the liver, while the greater omentum drapes over the intestines and contains fat deposits and lymph nodes.
Blood and Nerve Supply
The stomach receives blood from the celiac trunk and is innervated by sympathetic fibers (thoracic splanchnic nerves via the celiac plexus) and parasympathetic fibers (vagus nerve).
Microscopic Anatomy of the Stomach
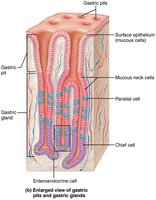
The stomach wall has four tunics, but the muscularis externa is unique in having three layers: longitudinal, circular, and oblique. This allows for effective churning and mixing of chyme. The mucosa is composed of simple columnar epithelium with mucous cells that secrete a protective alkaline mucus. The surface is dotted with gastric pits leading to gastric glands that produce gastric juice.

Types of Gland Cells
Mucous neck cells: Secrete thin, acidic mucus.
Parietal cells: Secrete hydrochloric acid (HCl) and intrinsic factor (for vitamin B12 absorption).
Chief cells: Secrete pepsinogen (inactive enzyme, activated to pepsin by HCl) and gastric lipase.
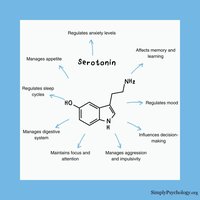
Enteroendocrine cells: Secrete hormones and paracrines (e.g., serotonin, histamine, somatostatin, gastrin).


Serotonin in the Gut
Although serotonin is widely known as a neurotransmitter in the brain, about 90-95% of the body's serotonin is produced in the gastrointestinal tract, where it regulates motility and secretion.
Mucosal Barrier
The stomach is protected from its harsh acidic environment by a mucosal barrier consisting of a thick layer of bicarbonate-rich mucus, tight junctions between epithelial cells, and rapid cell turnover (surface cells replaced every 3–6 days).
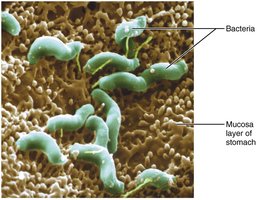
Clinical – Homeostatic Imbalance: Gastritis and Ulcers
Gastritis is inflammation of the stomach mucosa, often caused by a breach in the mucosal barrier. Peptic or gastric ulcers are erosions in the stomach wall, most commonly caused by Helicobacter pylori infection or NSAIDs (e.g., aspirin, ibuprofen). Severe ulcers can lead to peritonitis or hemorrhage.


Digestive Processes in the Stomach
The stomach performs mechanical and chemical digestion, serves as a food reservoir, and delivers chyme to the small intestine. HCl denatures proteins, and pepsin digests them. In infants, rennin digests milk protein. The only essential stomach function is the secretion of intrinsic factor for vitamin B12 absorption, necessary for red blood cell maturation.
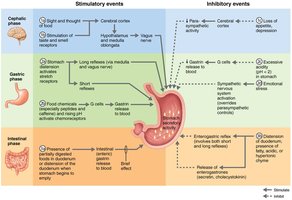
Regulation of Gastric Secretion
More than 3 liters of gastric juice are secreted daily, regulated by neural (vagus nerve increases, sympathetic decreases) and hormonal (gastrin stimulates HCl secretion) mechanisms. Gastric secretion occurs in three phases:
Cephalic (reflex) phase: Triggered by sight, smell, taste, or thought of food.
Gastric phase: Lasts 3–4 hours, accounts for most gastric juice. Stimulated by stomach distension and chemical stimuli (proteins, caffeine, low acidity).
Intestinal phase: Brief stimulation as chyme enters the duodenum, followed by inhibition to prevent overloading the intestine.
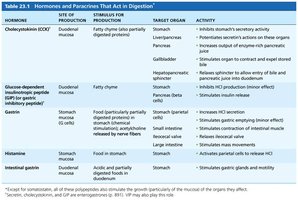
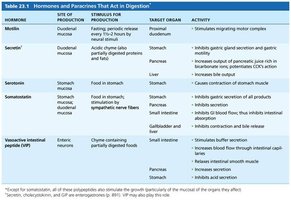
Hormones and Paracrines in Digestion
Hormone/Paracrine | Site of Production | Stimulus | Target Organ | Activity |
|---|---|---|---|---|
Cholecystokinin (CCK) | Duodenal mucosa | Fatty chyme | Stomach, Liver/Pancreas, Gallbladder | Inhibits gastric secretion, stimulates enzyme-rich pancreatic juice, stimulates gallbladder contraction |
Gastrin | Stomach mucosa | Food in stomach | Stomach, Small intestine, Ileocecal valve, Large intestine | Increases HCl secretion, stimulates contraction, relaxes ileocecal valve, stimulates mass movements |
Histamine | Stomach mucosa | Food in stomach | Stomach | Activates parietal cells to release HCl |
Secretin | Duodenal mucosa | Acidic chyme | Stomach, Pancreas, Liver | Inhibits gastric secretion, increases bile output |
Somatostatin | Stomach, duodenal mucosa | Food in stomach, sympathetic nerve fibers | Stomach, pancreas, small intestine, liver | Inhibits gastric secretion, inhibits GI blood flow, inhibits contraction and bile release |
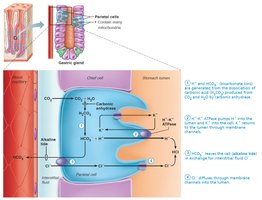
Mechanism of HCl Formation
Parietal cells secrete HCl by pumping H+ ions (from carbonic acid breakdown) into the stomach lumen via H+/K+ ATPase (proton pumps). Bicarbonate (HCO3−) is exported to the blood, causing an "alkaline tide." Chloride ions (Cl−) join H+ in the lumen to form HCl.
Equation for carbonic acid breakdown:
Regulation of Gastric Motility and Emptying
Stomach Filling and Contraction
The stomach stretches to accommodate food via receptive relaxation and gastric accommodation. Peristaltic waves (basic electrical rhythm set by pacemaker cells) move chyme toward the pylorus. Contractions are strongest near the pylorus, allowing only small amounts of chyme to enter the duodenum at a time.
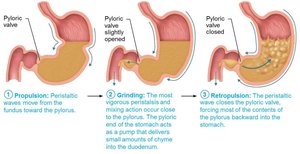
Regulation of Gastric Emptying
The duodenum regulates gastric emptying by responding to stretch and chemical signals. Enterogastric reflex and enterogastrones (secretin, CCK) inhibit gastric secretion and motility to prevent overfilling. Fatty chyme slows gastric emptying, while carbohydrate-rich chyme moves quickly.

Clinical – Homeostatic Imbalance: Vomiting
Vomiting (emesis) is triggered by extreme stretching or irritants and is coordinated by the emetic center in the medulla. Excessive vomiting can cause dehydration and metabolic alkalosis due to loss of stomach acid.
Liver, Gallbladder, and Pancreas
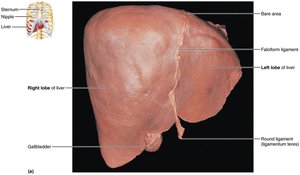
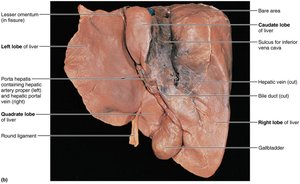
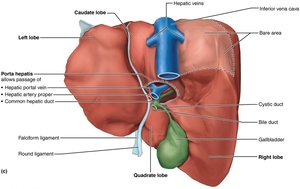
The Liver
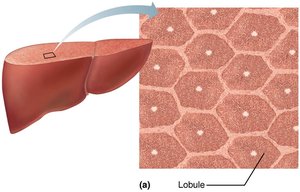
The liver is the largest gland in the body and has four lobes. It is suspended by the falciform ligament and receives blood via the hepatic artery and portal vein. The liver's main digestive function is the production of bile, which emulsifies fats.
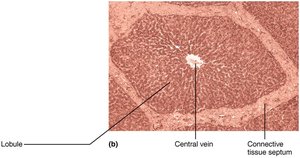
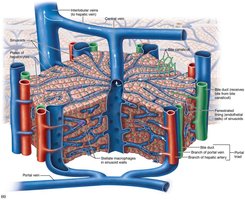
Microscopic Anatomy of the Liver
The liver is organized into lobules, hexagonal units made of hepatocytes. Each lobule has a central vein and portal triads (branch of hepatic artery, portal vein, and bile duct) at each corner. Blood flows through sinusoids past hepatocytes, which process nutrients and detoxify blood. Stellate macrophages remove debris and old RBCs.
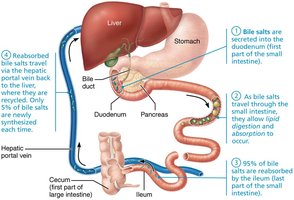
Bile: Composition and Enterohepatic Circulation
Bile is a yellow-green, alkaline fluid containing bile salts (for fat emulsification), bilirubin (a heme breakdown product), cholesterol, phospholipids, and electrolytes. Bile salts are recycled via the enterohepatic circulation: reabsorbed in the ileum, returned to the liver, and resecreted.
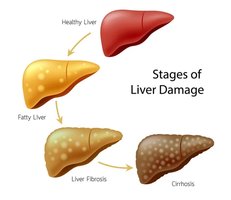
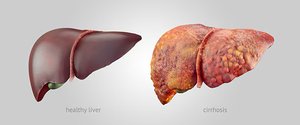
Homeostatic Imbalances of the Liver
Hepatitis: Inflammation, usually viral, but can be due to toxins or drugs.
Cirrhosis: Chronic inflammation leading to fibrosis and loss of function; can cause portal hypertension.
The liver can regenerate after significant loss of tissue.
The Gallbladder
The gallbladder stores and concentrates bile, releasing it into the duodenum via the cystic duct when needed, especially after a fatty meal. Removal of the gallbladder (cholecystectomy) requires dietary adjustments to reduce fat intake.
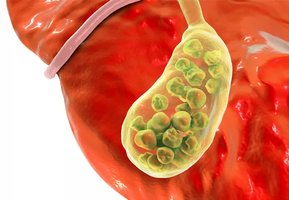
Clinical – Homeostatic Imbalance: Gallstones
Gallstones (biliary calculi) form when there is too much cholesterol or too few bile salts, potentially blocking bile flow and causing pain or jaundice. Treatment options include drugs, lithotripsy, or surgery.
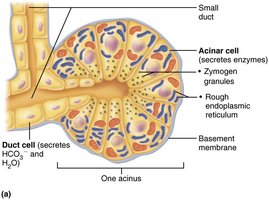
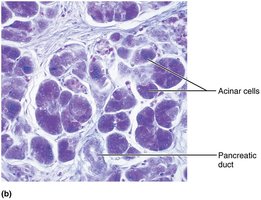
The Pancreas
The pancreas is both an exocrine and endocrine gland. Its exocrine function is to produce pancreatic juice (containing digestive enzymes and bicarbonate) that is delivered to the duodenum. The endocrine function involves secretion of insulin and glucagon by islet cells.
Composition and Activation of Pancreatic Juice
Pancreatic juice is alkaline (pH 8), neutralizing acidic chyme.
Contains enzymes: proteases (for proteins, secreted in inactive form), amylase (carbohydrates), lipases (lipids), nucleases (nucleic acids).
Proteases are activated in the duodenum by enteropeptidase (e.g., trypsinogen to trypsin).
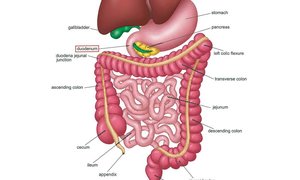
Bile and Pancreatic Secretion into the Small Intestine
The bile duct and pancreatic duct unite at the hepatopancreatic ampulla, opening into the duodenum. The hepatopancreatic sphincter regulates the entry of bile and pancreatic juice. Secretion is controlled by neural and hormonal signals, especially cholecystokinin (CCK) and secretin.
Summary Table: Hormones and Paracrines That Act in Digestion
Hormone | Site of Production | Stimulus | Target Organ | Activity |
|---|---|---|---|---|
Cholecystokinin (CCK) | Duodenal mucosa | Fatty chyme | Stomach, Liver/Pancreas, Gallbladder | Inhibits gastric secretion, stimulates enzyme-rich pancreatic juice, stimulates gallbladder contraction |
Gastrin | Stomach mucosa | Food in stomach | Stomach, Small intestine, Ileocecal valve, Large intestine | Increases HCl secretion, stimulates contraction, relaxes ileocecal valve, stimulates mass movements |
Secretin | Duodenal mucosa | Acidic chyme | Stomach, Pancreas, Liver | Inhibits gastric secretion, increases bile output |
Somatostatin | Stomach, duodenal mucosa | Food in stomach, sympathetic nerve fibers | Stomach, pancreas, small intestine, liver | Inhibits gastric secretion, inhibits GI blood flow, inhibits contraction and bile release |
Additional info: The notes above integrate and expand upon the provided material, ensuring a comprehensive, academically sound summary suitable for ANP college students.
