 Back
BackDiuretic Agents: Mechanisms, Classes, and Clinical Applications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Overview of Diuretic Agents
Diuretic agents are a diverse group of medications that increase the excretion of water and electrolytes from the body by acting on different segments of the nephron. They are essential in the management of various cardiovascular, renal, and metabolic disorders. This guide summarizes the pharmacology, mechanisms, clinical uses, and toxicities of major diuretic classes.
Carbonic Anhydrase Inhibitors
Mechanism of Action
Carbonic anhydrase inhibitors, such as acetazolamide, act primarily in the proximal convoluted tubule (PCT) by inhibiting the enzyme carbonic anhydrase. This enzyme catalyzes the reversible hydration of carbon dioxide and dehydration of carbonic acid, which is crucial for bicarbonate (HCO3-) reabsorption.
Effect: Inhibition leads to decreased HCO3- and Na+ reabsorption, resulting in increased urinary excretion of these ions and water (diuresis).
Clinical Applications: Rarely used as diuretics today, but important in glaucoma, urinary alkalinization, metabolic alkalosis, acute mountain sickness, and as adjuncts in epilepsy and other conditions.
Toxicities: Hyperchloremic metabolic acidosis, renal stones, potassium and phosphorus wasting, drowsiness, paresthesias, and hypersensitivity reactions.
Sodium Glucose Cotransporter 2 (SGLT2) Inhibitors
Mechanism of Action
SGLT2 inhibitors (e.g., dapagliflozin, canagliflozin) act in the proximal tubule to block glucose and sodium reabsorption, leading to glucosuria and natriuresis.
Effect: Increased urinary glucose and sodium excretion, mild diuretic effect, and reduction in blood pressure.
Clinical Applications: Third-line therapy for diabetes mellitus, with additional benefits in cardiac and renal protection.
Toxicities: Increased risk of genital fungal infections, urinary tract infections, and rare cases of acute kidney injury.
Loop Diuretics
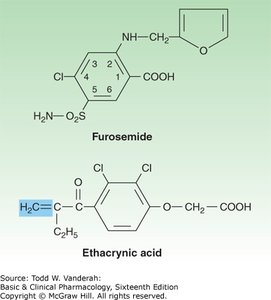
Chemistry and Prototypes
Loop diuretics, including furosemide, bumetanide, torsemide, and ethacrynic acid, are the most potent diuretics. They act on the thick ascending limb (TAL) of the loop of Henle.
Mechanism: Inhibit the Na+/K+/2Cl- cotransporter (NKCC2), reducing reabsorption of NaCl and diminishing the lumen-positive potential, which also increases Mg2+ and Ca2+ excretion.
Clinical Applications: Acute pulmonary edema, heart failure, hypercalcemia, hyperkalemia, acute renal failure, and anion overdose.
Toxicities: Hypokalemic metabolic alkalosis, ototoxicity, hyperuricemia, hypomagnesemia, allergic reactions (except ethacrynic acid), dehydration, and risk of fractures.
Thiazide and Thiazide-like Diuretics
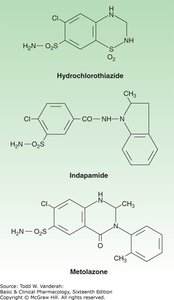
Chemistry and Prototypes
Thiazide diuretics, such as hydrochlorothiazide, chlorthalidone, and indapamide, act mainly in the distal convoluted tubule (DCT).
Mechanism: Inhibit the Na+/Cl- cotransporter (NCC), reducing NaCl reabsorption and enhancing Ca2+ reabsorption.
Clinical Applications: Hypertension, heart failure, nephrolithiasis due to hypercalciuria, and nephrogenic diabetes insipidus.
Toxicities: Hypokalemic metabolic alkalosis, impaired glucose tolerance, hyperlipidemia, hyponatremia, gout, allergic reactions, increased risk of skin cancer, and rare systemic effects.
Potassium-Sparing Diuretics
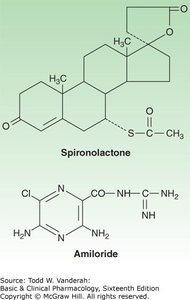
Mechanism of Action
Potassium-sparing diuretics act in the collecting tubules and ducts. They include aldosterone antagonists (spironolactone, eplerenone) and epithelial sodium channel blockers (amiloride, triamterene).
Effect: Reduce Na+ reabsorption and K+ secretion, preventing hypokalemia associated with other diuretics.
Clinical Applications: Hyperaldosteronism, heart failure, resistant hypertension, and conditions with secondary aldosteronism. Amiloride is also used in Liddle syndrome and lithium-induced nephrogenic diabetes insipidus.
Toxicities: Hyperkalemia, metabolic acidosis, gynecomastia (spironolactone), kidney stones (triamterene), and drug interactions.
Osmotic Diuretics
Mechanism of Action
Osmotic diuretics, such as mannitol, act in the proximal tubule and descending limb of Henle by increasing the osmolarity of the filtrate, thus retaining water in the tubule.
Clinical Applications: Reduction of intracranial and intraocular pressure, prevention of renal toxin accumulation, and management of acute renal failure.
Toxicities: Extracellular volume expansion, dehydration, hypernatremia, hyperkalemia, and risk of acute renal failure in susceptible patients.
Antidiuretic Hormone (ADH) Antagonists
Mechanism of Action
ADH antagonists (e.g., tolvaptan, conivaptan, demeclocycline, lithium) inhibit the action of ADH in the collecting tubule, promoting free water excretion (aquaretic effect).
Clinical Applications: Syndrome of inappropriate ADH secretion (SIADH), heart failure with hyponatremia, and autosomal dominant polycystic kidney disease.
Toxicities: Hypernatremia, nephrogenic diabetes insipidus, renal failure, and hepatotoxicity (tolvaptan).
Diuretic Combinations
Rationale and Clinical Use
Combining diuretics that act at different nephron sites can produce synergistic effects, especially in refractory edema or heart failure. Common combinations include loop diuretics with thiazides and potassium-sparing agents with loop or thiazide diuretics.
Loop + Thiazide: Used in diuretic resistance; requires careful monitoring for hypokalemia and volume status.
Potassium-Sparing + Other Diuretics: Used to prevent hypokalemia; caution in renal insufficiency due to risk of hyperkalemia.
Summary Table: Effects of Major Diuretic Classes
Class | Site of Action | Main Effect | Key Toxicity |
|---|---|---|---|
Carbonic Anhydrase Inhibitors | Proximal Tubule | NaHCO3 diuresis | Metabolic acidosis |
Loop Diuretics | Thick Ascending Limb | NaCl, K+, Ca2+, Mg2+ diuresis | Hypokalemia, ototoxicity |
Thiazides | Distal Convoluted Tubule | NaCl diuresis, Ca2+ retention | Hypokalemia, hyperglycemia |
Potassium-Sparing | Collecting Tubule/Duct | Na+ diuresis, K+ retention | Hyperkalemia |
Osmotic Diuretics | Proximal Tubule, Loop of Henle | Water diuresis | Volume expansion, dehydration |
ADH Antagonists | Collecting Tubule | Water diuresis (aquaretic) | Hypernatremia |
Additional info: This summary integrates foundational pharmacology with clinical applications and adverse effects, providing a comprehensive review suitable for ANP college-level study.
