 Back
BackDiuretics: Mechanisms, Sites of Action, and Clinical Implications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Introduction to Diuretics and Renal Physiology
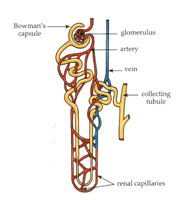
Overview of the Nephron
The nephron is the functional unit of the kidney, responsible for filtering blood, reabsorbing essential substances, and excreting waste. Diuretics act on different segments of the nephron to alter the reabsorption of ions and water, thereby increasing urine output.
Bowman's capsule surrounds the glomerulus, where filtration of blood occurs.
Most ions and small molecules are filtered, while protein-bound drugs are typically retained in the blood.
Reabsorption of ions and water occurs throughout the nephron, primarily via specialized transporters and channels.
Definitions and Key Concepts
Diuresis: Excretion of water in urine.
Natriuresis: Excretion of sodium (Na+) in urine.
Most diuretics promote natriuresis, leading to increased water loss because water follows sodium osmotically.
Key ions affected by diuretics: Na+, K+, HCO3-, Ca2+, Mg2+.
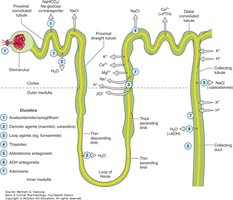
Classification of Diuretics
By Site of Action
Proximal tubule: Carbonic anhydrase inhibitors (e.g., acetazolamide)
Loop of Henle: Loop diuretics (e.g., furosemide, bumetanide)
Distal convoluted tubule: Thiazide diuretics (e.g., hydrochlorothiazide)
Collecting tubule: Potassium-sparing diuretics (e.g., spironolactone, amiloride)
By Mechanism
High ceiling (potent) diuretics: Loop diuretics
Thiazide diuretics: Moderate potency, act on distal tubule
K+-sparing diuretics: Act on collecting tubule, prevent K+ loss
Renal Ion Transport Mechanisms
Primary and Secondary Active Transport
Ion movement in the nephron is driven by active and passive mechanisms:
Primary active transport: Direct use of ATP, e.g., Na+/K+ ATPase pump moves 3 Na+ out of the cell and 2 K+ into the cell against their gradients.
Secondary active transport: Uses the energy from one ion moving down its gradient to drive another ion against its gradient. Includes symporters (cotransporters) and antiporters (exchangers).

Ion Channels and Facilitated Diffusion
Ion channels allow ions to move down their concentration and electrical gradients without energy input.
Facilitated diffusion is mediated by membrane proteins and does not require ATP.
Proximal Convoluted Tubule (PCT) and Carbonic Anhydrase Inhibitors
Physiology of the PCT
The PCT is responsible for the majority of Na+, HCO3-, and water reabsorption. Carbonic anhydrase (CA) plays a key role in bicarbonate reabsorption.
Na+/K+ pump maintains low intracellular Na+.
CA catalyzes the conversion of H2CO3 to CO2 and H2O, which diffuse into the cell and are reconverted to HCO3-.
Na+ reabsorption is coupled to H+ secretion via antiporters.

Carbonic Anhydrase Inhibitors (e.g., Acetazolamide)
Mechanism: Inhibit CA, reducing HCO3- and Na+ reabsorption.
Effects: Increased excretion of HCO3- and Na+, leading to metabolic acidosis and mild diuresis.
Indications: Glaucoma, acute mountain sickness, metabolic alkalosis (rarely as a diuretic).
Side effects: Metabolic acidosis, renal stones, paresthesia, sulfa allergy, hypokalemia.
Loop of Henle and Loop Diuretics
Thick Ascending Limb Physiology
The thick ascending limb reabsorbs Na+, K+, and Cl- via the Na+/K+/2Cl- cotransporter (NKCC2). This segment is impermeable to water.
Na+ reabsorption creates a positive lumen potential, driving paracellular reabsorption of Mg2+ and Ca2+.
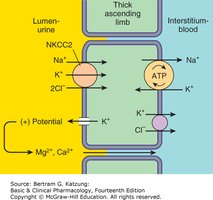
Loop Diuretics (e.g., Furosemide, Bumetanide)
Mechanism: Inhibit NKCC2, blocking Na+, K+, and Cl- reabsorption.
Effects: Increased excretion of Na+, K+, Cl-, Mg2+, and Ca2+; potent diuresis.
Indications: Pulmonary edema, heart failure, hypercalcemia, hyperkalemia, acute renal failure.
Side effects: Dehydration, hyponatremia, hypokalemia, hypomagnesemia, metabolic alkalosis, hyperuricemia, ototoxicity, sulfa allergy.
Distal Convoluted Tubule (DCT) and Thiazide Diuretics
DCT Physiology
The DCT reabsorbs Na+ and Cl- via the Na+/Cl- cotransporter and is a key site for Ca2+ reabsorption, regulated by parathyroid hormone (PTH).
Thiazide diuretics increase Ca2+ reabsorption by enhancing the Na+/Ca2+ exchanger on the basolateral membrane.

Thiazide Diuretics (e.g., Hydrochlorothiazide)
Mechanism: Inhibit Na+/Cl- cotransporter, reducing Na+ reabsorption.
Effects: Mild diuresis, increased Ca2+ reabsorption, ceiling effect (limited maximal efficacy).
Indications: Hypertension, edema, nephrolithiasis due to hypercalciuria.
Side effects: Hyponatremia, dehydration, hypokalemia, metabolic alkalosis, hyperglycemia, hyperlipidemia, hyperuricemia, hypercalcemia.
Collecting Tubule and Potassium-Sparing Diuretics
Collecting Tubule Physiology
The collecting tubule is the final site for Na+ reabsorption and K+ and H+ secretion. Aldosterone increases Na+ channel (ENaC) expression and Na+/K+ ATPase activity, while antidiuretic hormone (ADH) regulates water reabsorption via aquaporins.

Potassium-Sparing Diuretics
Spironolactone, Eplerenone: Aldosterone receptor antagonists; decrease Na+ reabsorption and K+ excretion.
Amiloride, Triamterene: Block ENaC channels directly; reduce Na+ reabsorption and K+ loss.
Indications: Ascites, hyperaldosteronism, hypertension, adjunct to other diuretics to prevent hypokalemia.
Side effects: Hyperkalemia, anti-androgenic effects (spironolactone).
Other Diuretic Mechanisms
Osmotic diuretics (e.g., mannitol): Increase osmolarity of tubular fluid, reducing water reabsorption. Used for cerebral edema and toxin elimination.
ADH antagonists (e.g., tolvaptan): Block vasopressin receptors, reducing water reabsorption in the collecting duct.
Summary Table: Diuretic Classes, Sites, and Effects
Class | Site of Action | Main Effect | Key Side Effects |
|---|---|---|---|
Carbonic Anhydrase Inhibitors | Proximal Tubule | ↑ Na+, HCO3- excretion | Metabolic acidosis, renal stones |
Loop Diuretics | Thick Ascending Limb | ↑ Na+, K+, Cl-, Ca2+, Mg2+ excretion | Hypokalemia, ototoxicity, metabolic alkalosis |
Thiazide Diuretics | Distal Convoluted Tubule | ↑ Na+, Cl- excretion, ↑ Ca2+ reabsorption | Hypercalcemia, hyperglycemia, metabolic alkalosis |
K+-Sparing Diuretics | Collecting Tubule | ↓ K+ excretion, mild diuresis | Hyperkalemia, gynecomastia (spironolactone) |
Osmotic Diuretics | Entire Nephron | ↑ H2O excretion | Dehydration, electrolyte imbalance |
Key Equations
Na+/K+ ATPase stoichiometry:
Carbonic anhydrase reaction:
Clinical Applications and Side Effects
Diuretics are used to manage hypertension, edema, heart failure, and certain electrolyte disorders.
Common side effects include electrolyte imbalances (e.g., hypokalemia, hyperkalemia), metabolic alkalosis or acidosis, and specific drug-related toxicities.
Understanding the site and mechanism of action is essential for predicting therapeutic effects and adverse reactions.
