Back
Backch 18 Electrical and Mechanical Events of the Heart: Cardiac Physiology and Regulation pt 2
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Cardiovascular System: Electrical and Mechanical Events of the Heart
Electrical Events of the Heart
The heart's ability to contract and pump blood is governed by a specialized conduction system that generates and distributes electrical impulses. This system ensures the heart beats in a coordinated and rhythmic manner, independent of direct nervous system stimulation, though it can be modulated by autonomic input.
Gap Junctions: Specialized connections between cardiac muscle cells that allow rapid transmission of electrical impulses.
Intrinsic Cardiac Conduction System: A network of noncontractile (autorhythmic) cells that initiate and distribute impulses, coordinating depolarization and contraction.
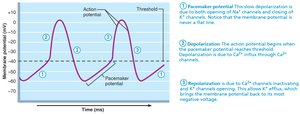
Pacemaker Cells and Action Potentials
Pacemaker cells, primarily located in the sinoatrial (SA) node, have unstable resting membrane potentials, known as pacemaker potentials or prepotentials. Their action potential consists of three main phases:
Pacemaker Potential: Slow depolarization due to opening of Na+ channels and closing of K+ channels.
Depolarization: Ca2+ channels open at threshold (around -40 mV), causing a rapid influx of Ca2+ and a sharp rise in membrane potential.
Repolarization: K+ channels open, allowing K+ efflux, returning the cell to a more negative membrane potential.
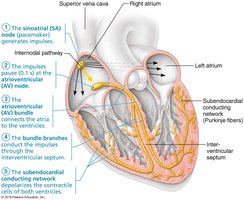
Sequence of Excitation in the Intrinsic Conduction System
The sequence of excitation ensures the heart contracts in a coordinated manner:
Sinoatrial (SA) Node: Pacemaker in the right atrial wall; initiates impulses (~75/minute).
Atrioventricular (AV) Node: Located in the inferior interatrial septum; delays impulse by ~0.1 second to allow atrial contraction.
AV Bundle (Bundle of His): Only electrical connection between atria and ventricles.
Right and Left Bundle Branches: Pathways in the interventricular septum toward the apex.
Subendocardial Conducting Network (Purkinje Fibers): Distributes impulse through ventricular walls, causing coordinated ventricular contraction.
Autonomic Innervation of the Heart
The autonomic nervous system (ANS) modulates heart rate and force of contraction:
Cardioacceleratory Center: Sympathetic stimulation increases heart rate and contractility.
Cardioinhibitory Center: Parasympathetic (vagus nerve) stimulation decreases heart rate.

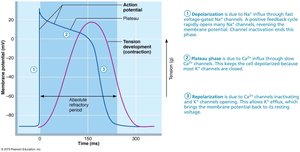
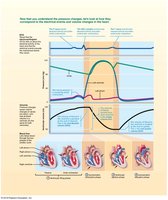
Action Potentials of Contractile Cardiac Muscle Cells
Contractile cardiac muscle fibers generate action potentials that differ from skeletal muscle, featuring a plateau phase that prolongs contraction and prevents tetanus.
Depolarization: Rapid Na+ influx through voltage-gated channels.
Plateau Phase: Slow Ca2+ influx keeps the cell depolarized.
Repolarization: Ca2+ channels inactivate, K+ channels open, restoring resting potential.
Cardiac muscle action potentials last about 200 ms, much longer than skeletal muscle, ensuring efficient blood ejection and preventing tetanic contractions.
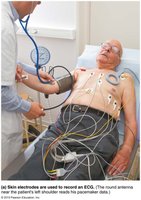
Electrocardiography (ECG/EKG)
An electrocardiogram (ECG) records the electrical activity of the heart, providing valuable diagnostic information. It is a composite of all action potentials generated by nodal and contractile cells at a given time.
P wave: Atrial depolarization (SA node activity).
QRS complex: Ventricular depolarization and atrial repolarization.
T wave: Ventricular repolarization.
P-R interval: Start of atrial to start of ventricular excitation.
S-T segment: Entire ventricular myocardium depolarized.
Q-T interval: Start of ventricular depolarization to end of repolarization.

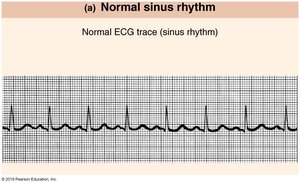
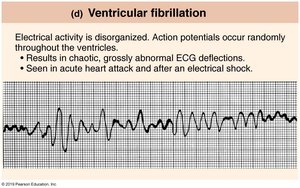
Normal and Abnormal ECG Tracings
ECG analysis can reveal normal sinus rhythm and various arrhythmias:
ECG Pattern | Description |
|---|---|
Normal Sinus Rhythm | Regular P, QRS, and T waves; normal heart rhythm. |
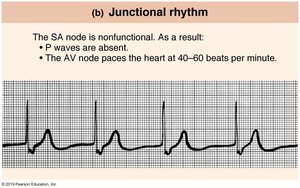
Junctional Rhythm | No P waves; AV node paces heart at 40–60 bpm. |
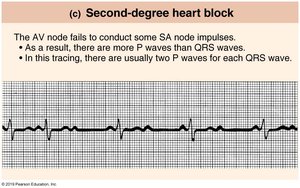
Second-degree Heart Block | More P waves than QRS complexes; some impulses not conducted. |
Ventricular Fibrillation | Disorganized electrical activity; chaotic ECG; seen in acute heart attack or after shock. |
Mechanical Events of the Heart: The Cardiac Cycle
The cardiac cycle describes the sequence of mechanical events during one heartbeat, including periods of contraction (systole) and relaxation (diastole). It ensures efficient blood flow through the heart and to the body.
Ventricular Filling (mid-to-late diastole): Blood flows passively into ventricles; atrial contraction delivers final 20% of blood (EDV).
Isovolumetric Contraction: Ventricles contract with all valves closed; pressure rises until SL valves open.
Ventricular Ejection: Blood is pumped into aorta and pulmonary trunk.
Isovolumetric Relaxation (early diastole): Ventricles relax, SL valves close, and pressure drops (ESV).
The cardiac cycle lasts about 0.8 seconds at a heart rate of 75 bpm.

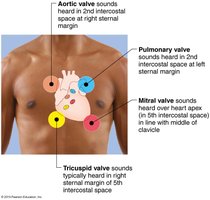
Heart Sounds
Two main heart sounds are produced by valve closures:
First sound (lub): Closing of AV valves at the start of ventricular systole.
Second sound (dup): Closing of SL valves at the start of ventricular diastole.
Valve sounds can be auscultated at specific chest locations.
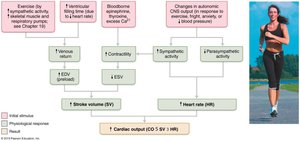
Regulation of Cardiac Output
Cardiac output (CO) is the volume of blood pumped by each ventricle per minute. It is determined by heart rate (HR) and stroke volume (SV):
Stroke Volume (SV): Volume of blood pumped per beat;
Cardiac Reserve: Difference between resting and maximal CO.
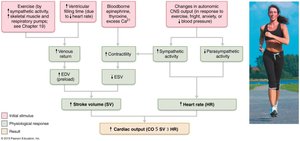
Regulation of Stroke Volume
Preload: Degree of stretch of cardiac muscle before contraction; increased by venous return (Frank-Starling law).
Contractility: Contractile strength at a given muscle length; increased by sympathetic stimulation and positive inotropic agents.
Afterload: Pressure ventricles must overcome to eject blood; increased by hypertension.

Regulation of Heart Rate
Autonomic Nervous System: Sympathetic stimulation increases HR; parasympathetic (vagal) stimulation decreases HR.
Chemicals: Hormones (epinephrine, thyroxine) and ions (Ca2+, K+) affect HR.
Other Factors: Age, gender, exercise, and body temperature influence HR.
Homeostatic Imbalances of Cardiac Output
Tachycardia: Abnormally fast HR (>100 bpm); may lead to fibrillation.
Bradycardia: Abnormally slow HR (<60 bpm); may be normal in athletes but pathological otherwise.
Congestive Heart Failure (CHF): Inadequate CO due to weakened myocardium; can result from coronary atherosclerosis, hypertension, myocardial infarcts, or dilated cardiomyopathy.
Pulmonary Congestion: Left-sided heart failure; blood backs up in lungs.
Peripheral Congestion: Right-sided heart failure; blood pools in body organs, causing edema.
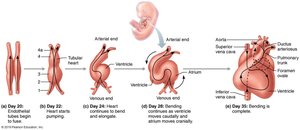
Developmental Aspects of the Heart
The heart develops from mesoderm, beginning as two endothelial tubes that fuse and form a single pumping chamber by day 22 of embryonic development. The heart tube undergoes complex folding and partitioning to form a four-chambered heart by day 35.
Sinus Venosus: Forms right atrium, coronary sinus, and SA node.
Atrium: Forms pectinate muscles of atria.
Ventricle: Forms left ventricle.
Bulbus Cordis: Forms aorta, pulmonary trunk, and right ventricle.
Fetal heart structures bypass pulmonary circulation:
Foramen Ovale: Connects atria; becomes fossa ovalis after birth.
Ductus Arteriosus: Connects pulmonary trunk to aorta; becomes ligamentum arteriosum after birth.