 Back
BackFemale Reproductive System: Ovarian and Uterine Cycles, Hormonal Regulation, and Sexually Transmitted Diseases
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Female Reproductive System
Hormonal Interactions During the Ovarian Cycle
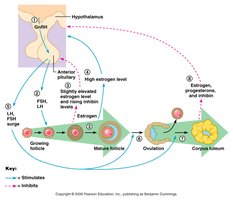
The ovarian cycle is regulated by a complex interplay of hormones that control follicle development, ovulation, and corpus luteum function. The hypothalamus, anterior pituitary, and ovaries communicate through feedback mechanisms to ensure proper timing and coordination of the cycle.
GnRH (Gonadotropin-Releasing Hormone): Released from the hypothalamus, it stimulates the anterior pituitary to secrete FSH and LH.
FSH (Follicle-Stimulating Hormone) and LH (Luteinizing Hormone): Promote follicle growth and maturation, and stimulate low-level estrogen production.
Estrogen: Rising levels initially inhibit FSH and LH release (negative feedback), but high levels later trigger a surge in LH (positive feedback).
LH Surge: Induces completion of meiosis I in the primary oocyte, triggers ovulation, and transforms the ruptured follicle into the corpus luteum.
Corpus Luteum: Secretes inhibin, progesterone, and estrogen, which suppress FSH and LH release and maintain the luteal phase.
Cycle Reset: Decline in ovarian hormones at the end of the cycle removes inhibition, allowing FSH and LH to rise and a new cycle to begin.
Feedback Mechanisms in Ovarian Function
Feedback loops between the hypothalamus, pituitary, and ovaries regulate the secretion of gonadotropins and ovarian hormones. Negative feedback predominates during most of the cycle, while positive feedback occurs just before ovulation.
Negative Feedback: Moderate estrogen and inhibin levels suppress FSH and LH secretion.
Positive Feedback: High estrogen levels stimulate a surge in LH, leading to ovulation.
Uterine (Menstrual) Cycle
Phases of the Uterine Cycle
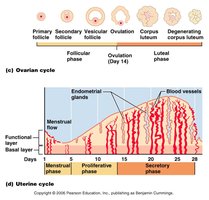
The uterine cycle describes the monthly changes in the endometrial lining of the uterus in response to fluctuating ovarian hormones. It is divided into three main phases:
Menstrual Phase (Days 1–5): The functional layer of the endometrium is shed, resulting in menstrual bleeding.
Proliferative (Preovulatory) Phase (Days 6–14): The endometrium rebuilds itself under the influence of rising estrogen levels.
Secretory (Postovulatory) Phase (Days 15–28): The endometrium prepares for possible embryo implantation, driven by progesterone from the corpus luteum.
Menses
If fertilization does not occur, progesterone levels fall, depriving the endometrium of hormonal support. This leads to constriction and spasm of spiral arteries, cell death, and eventual sloughing of the functional layer as menstrual flow.
Spiral Arteries: Undergo cycles of constriction and relaxation, leading to breakdown of the endometrial tissue.
Functional Layer: Is shed during menstruation, while the basal layer remains to regenerate the endometrium.
Hormonal Fluctuations During the Ovarian and Uterine Cycles
Gonadotropin and Ovarian Hormone Levels
Hormone levels fluctuate in a predictable pattern throughout the ovarian and uterine cycles, coordinating follicular development, ovulation, and endometrial changes.
Gonadotropins (FSH and LH): FSH rises early to stimulate follicle growth; LH surges mid-cycle to trigger ovulation.
Ovarian Hormones (Estrogen and Progesterone): Estrogen peaks before ovulation; progesterone rises after ovulation during the luteal phase.

Extrauterine Effects of Estrogens and Progesterone
Estrogen Effects
Estrogens have widespread effects beyond the reproductive organs, especially during puberty and reproductive years.
Oogenesis and Follicle Growth: Stimulate development of oocytes and ovarian follicles.
Anabolic Effects: Promote growth and functional maturation of the uterine tubes, uterus, and vagina.
Motility: Enhance motility of the uterine tubes and uterus.
Secondary Sex Characteristics: Include breast development, increased subcutaneous fat (hips and breasts), widening of the pelvis, and growth of axillary and pubic hair.
Female Sexual Response
Physiological Changes
Sexual arousal in females involves increased blood flow to the clitoris, vaginal mucosa, and breasts, as well as lubrication of the vestibule. Orgasm is characterized by muscle tension, increased heart rate and blood pressure, and rhythmic uterine contractions.
Multiple Orgasms: Females do not have a refractory period and may experience multiple orgasms in one sexual encounter.
Conception: Orgasm is not required for fertilization to occur.
Sexually Transmitted Diseases (STDs)
Gonorrhea
Gonorrhea is a bacterial infection transmitted through mucosal contact. It can cause painful urination and discharge in males, and may be asymptomatic or cause pelvic inflammatory disease in females. Antibiotic resistance is an increasing concern.
Syphilis
Syphilis is a bacterial infection that can be transmitted sexually or congenitally. It progresses through primary (chancre), secondary (rash, fever, joint pain), latent, and tertiary (gummas) stages. Penicillin is the treatment of choice.
Chlamydia
Chlamydia is the most common STD in the U.S., responsible for a significant proportion of pelvic inflammatory disease cases. It can cause urethritis, discharge, pain, and infertility. Treated with tetracycline antibiotics.
Viral Infections
Genital Warts: Caused by human papillomavirus (HPV), associated with increased risk of genital cancers.
Genital Herpes: Caused by Epstein-Barr virus type 2, characterized by latent periods and flare-ups. Congenital infection can cause fetal malformations. Treated with antiviral drugs such as acyclovir.
