 Back
BackFluid and Electrolyte Balance: Water and Sodium Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Fluid and Electrolyte Balance
Introduction to Fluid and Electrolyte Balance
Fluid and electrolyte balance is essential for maintaining homeostasis in the human body. The kidneys play a central role in regulating both the volume and composition of body fluids, particularly plasma, by controlling solute and water content. This regulation is crucial for maintaining mean arterial pressure (MAP) and proper cellular function.
Input and Output: Fluid and electrolytes enter the body through ingestion and are lost via excretion, sweating, hemorrhage, and respiration.
Production and Utilization: Cellular metabolism also contributes to water production and utilization.
Key Organs: The kidneys are the only organs that regulate water excretion for the sake of balance.
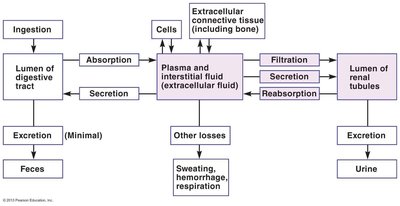
Material Exchanges Affecting Plasma Content
Material exchanges between the digestive tract, cells, extracellular fluid, and renal tubules determine plasma composition. The kidneys regulate plasma volume and osmolarity by adjusting filtration, secretion, and reabsorption processes.
Absorption: Movement of substances from the digestive tract into plasma and interstitial fluid.
Filtration, Secretion, Reabsorption: Processes in the kidneys that determine the final composition of urine and plasma.
Other Losses: Include sweating, hemorrhage, and respiration.
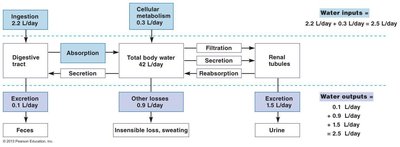
Water Balance
Water balance is achieved when water input equals water output. The kidneys are responsible for adjusting water reabsorption to maintain this balance, which is vital for plasma volume and osmolarity.
Water Inputs: Ingestion (2.2 L/day) and cellular metabolism (0.3 L/day) provide a total of 2.5 L/day.
Water Outputs: Feces (0.1 L/day), insensible loss and sweating (0.9 L/day), and urine (1.5 L/day) sum to 2.5 L/day.
Effects of Water Balance on Plasma Volume and Osmolarity
Changes in plasma volume affect MAP, while changes in plasma osmolarity influence fluid movement between compartments (intracellular vs. extracellular fluid). Conditions such as hypervolemia, hypovolemia, and dehydration can disrupt homeostasis.
Exercise and Sweating: Lead to water and electrolyte loss, increasing plasma osmolarity and signaling the kidneys to reabsorb water.
Dehydration: Decreases plasma osmolarity, causing neuron swelling and headaches; kidneys are signaled to excrete water.
Hyperhydration: Excess water intake can dilute plasma osmolarity, also affecting kidney function.
Renal Handling of Water
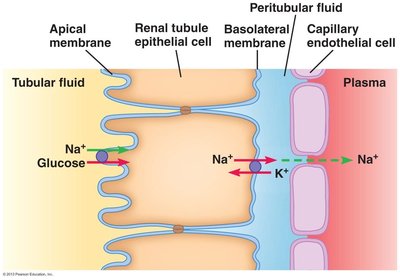
Water Reabsorption in the Nephron
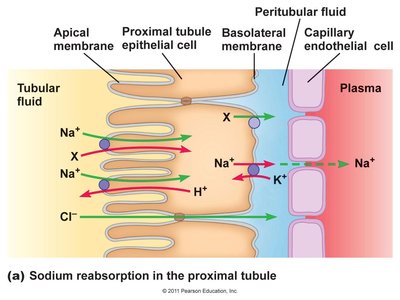
The kidneys adjust water reabsorption to maintain plasma volume and osmolarity. Water is never secreted, only filtered and reabsorbed. The osmotic gradient, primarily established by sodium (Na+), drives water reabsorption.
Proximal Tubule: 70% of Na+ is reabsorbed here, and water follows by osmosis.
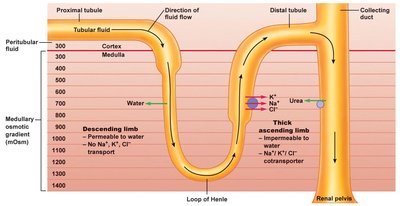
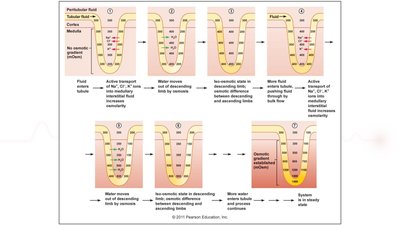
Water Reabsorption in the Loop of Henle
The loop of Henle, especially in juxtamedullary nephrons, establishes a medullary osmotic gradient (from 300 mOsm in the cortex to 1200–1400 mOsm in the inner medulla). This gradient is essential for water reabsorption and urine concentration.
Descending Limb: Permeable to water, but not to Na+, K+, or Cl-.
Thick Ascending Limb: Impermeable to water; actively transports Na+, K+, and Cl- out of the tubule.
Countercurrent Multiplier: Establishes the osmotic gradient; urea recycling helps maintain it.
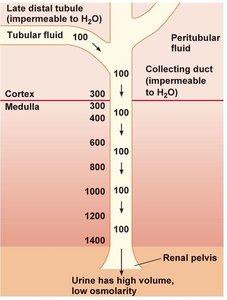
Water Reabsorption in the Distal Convoluted Tubule (DCT) and Collecting Duct
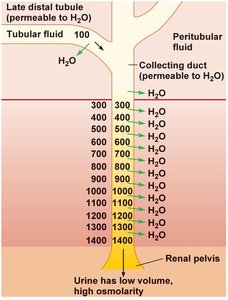
The permeability of the late DCT and collecting duct to water is regulated by hormones. When these segments are impermeable to water, urine is dilute and of high volume. When permeable, urine is concentrated and of low volume.
"Tight" Tight Junctions: Prevent water movement unless aquaporins are present.
Hormonal Regulation: Antidiuretic hormone (ADH) increases water permeability by stimulating aquaporin insertion.
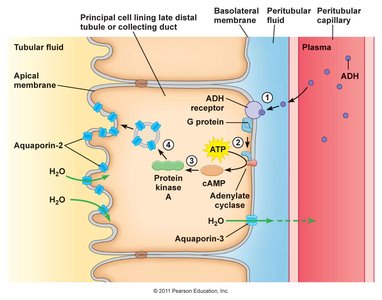
Role of Aquaporins and ADH
Aquaporins are water channels required for water reabsorption in the late DCT and collecting duct. ADH (antidiuretic hormone) regulates the insertion of aquaporin-2 channels into the apical membrane, increasing water reabsorption.
ADH Mechanism: Binds to receptors, activates cAMP, and promotes aquaporin-2 insertion.
Regulation of ADH Secretion
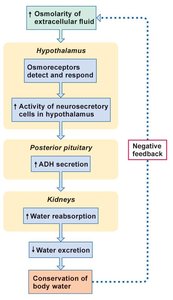
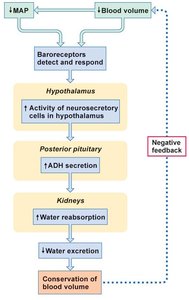
ADH secretion is regulated by plasma osmolarity and blood volume. Osmoreceptors in the hypothalamus and baroreceptors in the cardiovascular system detect changes and adjust ADH release accordingly.
Increased Osmolarity: Stimulates ADH release, increasing water reabsorption and conserving body water.
Decreased Blood Volume or MAP: Also stimulates ADH release to conserve blood volume.
Sodium (Na+) Balance
Importance of Sodium
Sodium is the primary solute in extracellular fluid (ECF) and is crucial for cellular excitation and the transport of other solutes. Sodium balance is tightly regulated because it affects plasma volume and osmolarity.
Hypernatremia: High plasma Na+ concentration.
Hyponatremia: Low plasma Na+ concentration.
Regulation: Na+ is freely filtered and reabsorbed, but not secreted, in the nephron.
Aldosterone and Sodium Reabsorption
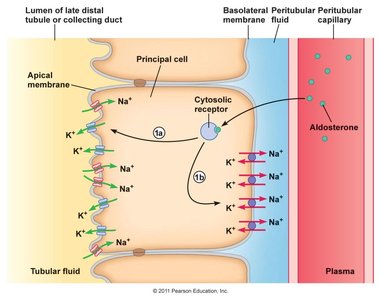
Aldosterone is a steroid hormone released from the adrenal cortex in response to angiotensin II (ANG II). It increases sodium reabsorption in the late distal tubule and collecting duct by stimulating the synthesis of Na+ channels and Na+/K+ pumps.
Mechanism: Aldosterone binds to cytosolic receptors, increasing transcription of sodium transport proteins.
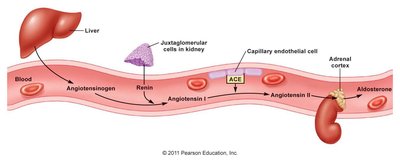
Renin-Angiotensin-Aldosterone System (RAAS)
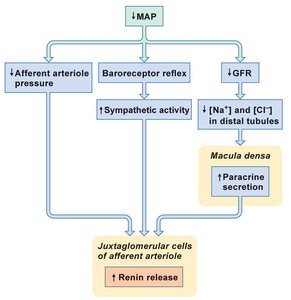
The RAAS is a hormone cascade pathway that helps regulate blood pressure and sodium balance. Low blood pressure stimulates renin release from juxtaglomerular cells, leading to the production of angiotensin II, which increases aldosterone secretion.
Key Steps: Renin converts angiotensinogen to angiotensin I, which is then converted to angiotensin II by ACE (angiotensin-converting enzyme).
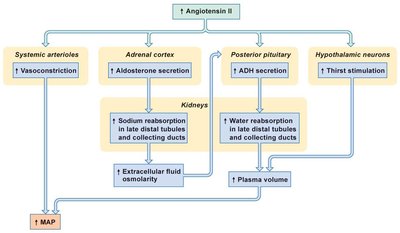
Effects: Angiotensin II causes vasoconstriction, stimulates aldosterone and ADH secretion, and increases thirst.
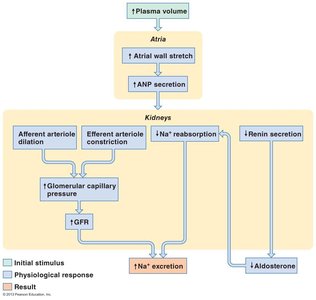
Atrial Natriuretic Peptide (ANP) and Sodium Regulation
ANP is a peptide hormone secreted by the atrial walls in response to increased plasma volume (atrial stretch). It promotes natriuresis (increased sodium excretion) by dilating afferent arterioles, constricting efferent arterioles, and inhibiting renin and aldosterone secretion.
Result: Increased sodium and water excretion, reducing plasma volume and blood pressure.
Summary Table: Hormonal Regulation of Water and Sodium Balance
Hormone | Stimulus | Target | Effect |
|---|---|---|---|
ADH | ↑ Plasma osmolarity, ↓ Blood volume | Late DCT & Collecting Duct | ↑ Water reabsorption |
Aldosterone | ↑ Angiotensin II, ↓ Na+ | Late DCT & Collecting Duct | ↑ Na+ reabsorption |
ANP | ↑ Plasma volume (atrial stretch) | Kidneys | ↑ Na+ excretion |
Additional info: The above notes integrate and expand upon the provided lecture slides, including definitions, mechanisms, and clinical relevance for ANP college-level physiology students.
