 Back
BackFluid, Electrolyte, and Acid-Base Balance: Structured Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Fluid, Electrolyte, and Acid-Base Balance
Body Fluids and Fluid Compartments
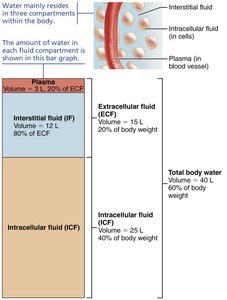
The human body is composed largely of water, distributed among various compartments. Understanding these compartments is essential for grasping fluid and electrolyte balance.
Total Body Water: Varies with age, sex, and body composition. Infants have the highest percentage (~73%), while elderly individuals have the lowest (~45%). Adult males average ~60%, and adult females ~50% due to differences in muscle and fat content.
Major Fluid Compartments:
Intracellular Fluid (ICF): Fluid within cells; accounts for about 2/3 of total body water (~25 L in adults).
Extracellular Fluid (ECF): Fluid outside cells; about 1/3 of total body water (~15 L). Subdivided into:
Plasma: Fluid portion of blood (~3 L).
Interstitial Fluid (IF): Fluid between cells (~12 L).
Other minor compartments: lymph, cerebrospinal fluid, synovial fluid, serous fluid, and gastrointestinal secretions (usually considered part of IF).
Composition of Body Fluids
Body fluids contain water (the universal solvent) and solutes, which are classified as electrolytes or nonelectrolytes.
Nonelectrolytes: Mostly organic molecules (e.g., glucose, lipids, urea) that do not dissociate in water and thus do not conduct electricity.
Electrolytes: Compounds that dissociate into ions in water (e.g., salts, acids, bases, some proteins). They have greater osmotic power than nonelectrolytes because they produce more particles per molecule.
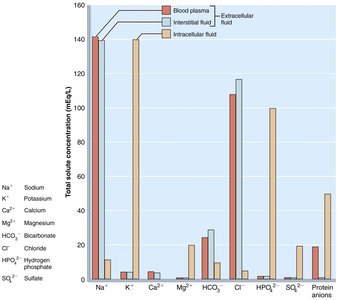
Electrolyte Distribution: Each compartment has a unique pattern of electrolytes:
ECF: Major cation is Na+; major anion is Cl−.
ICF: Major cation is K+; major anion is HPO42− (hydrogen phosphate).
Proteins, phospholipids, cholesterol, and triglycerides constitute the greatest mass of dissolved solutes, especially in ICF.
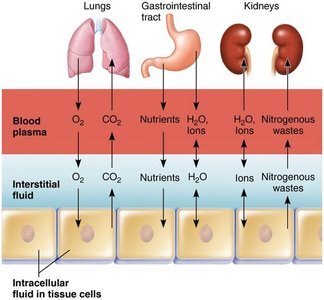
Fluid Movement Among Compartments
There is continuous exchange and mixing of body fluids, primarily regulated by osmotic and hydrostatic pressures.
Water Movement: Water moves freely between compartments along osmotic gradients. Solutes, especially large or charged ones, move less freely.
Capillary Exchange: Plasma and IF exchange occurs across capillary walls; most fluid lost at the arteriolar end is reabsorbed at the venule end, with lymphatics returning excess fluid to the blood.
Cell Membrane Exchange: IF and ICF exchange occurs across plasma membranes, with selective ion movement and two-way osmotic flow of water.
Water Balance and Regulation
Water Intake and Output
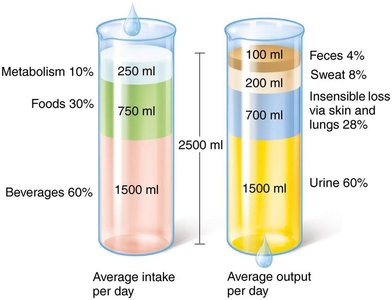
Water balance is maintained when intake equals output, averaging about 2500 ml/day in adults.
Sources of Water Intake:
Beverages (60%)
Foods (30%)
Metabolic water (10%)—produced by cellular metabolism
Routes of Water Output:
Urine (60%)
Insensible loss via skin and lungs (28%)
Sweat (8%)
Feces (4%)
Regulation of Water Intake
The hypothalamic thirst center regulates water intake, responding to changes in plasma osmolality, dry mouth, and blood volume/pressure.
Stimuli for Thirst:
Increased plasma osmolality (detected by hypothalamic osmoreceptors)
Decreased saliva production (dry mouth)
Decreased blood volume or pressure (via angiotensin II or baroreceptor input)
Inhibitory Feedback: Drinking water relieves thirst by moistening the mouth and activating stretch/osmoreceptors in the GI tract.

Regulation of Water Output
Water output is regulated mainly by the kidneys, which adjust urine volume and concentration in response to fluid intake, diet, and water loss via sweat and feces.
Obligatory Water Losses: Insensible loss (skin, lungs), urine (minimum 500 ml/day), sweat, and feces.
Role of Antidiuretic Hormone (ADH):
ADH increases water reabsorption in the collecting ducts, reducing urine output and increasing body fluid volume.
ADH release is stimulated by increased ECF osmolality (primary), decreased blood volume/pressure, and other stressors (e.g., severe blood loss, burns).
Decreased ADH leads to increased urine output and decreased body fluid volume.

Disorders of Water Balance
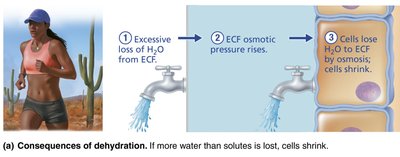
Dehydration
Dehydration results from excessive loss of water from the ECF, leading to cell shrinkage and impaired function.
Causes: Hemorrhage, burns, vomiting, diarrhea, sweating, water deprivation, diuretic abuse, endocrine disturbances.
Symptoms: Thirst, dry mouth, flushed skin, reduced urine output, weight loss, confusion, hypovolemic shock.
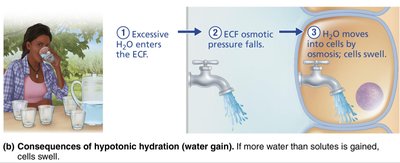
Hypotonic Hydration (Water Intoxication)
Hypotonic hydration occurs when water intake exceeds water loss, diluting ECF and causing cells to swell.
Causes: Renal insufficiency, rapid excess water ingestion.
Consequences: Hyponatremia, cerebral edema, nausea, vomiting, muscle cramps, convulsions, death if severe.
Edema
Edema is the accumulation of fluid in the interstitial space, leading to tissue swelling (not cell swelling).
Causes: Increased capillary hydrostatic pressure, decreased plasma protein levels, lymphatic obstruction, increased capillary permeability.
Consequences: Impaired tissue function due to increased diffusion distance for oxygen and nutrients.
Electrolyte Balance
Major Electrolytes and Their Regulation
Electrolyte balance is crucial for fluid movement, cell excitability, and metabolic processes. The main ions regulated are sodium, potassium, calcium, and phosphate.
Sodium (Na+): Most abundant ECF cation; regulates ECF volume, blood pressure, and water distribution.
Potassium (K+): Most abundant ICF cation; essential for resting membrane potential and neuromuscular function.
Calcium (Ca2+): Important for bone structure, blood clotting, muscle contraction, and nerve function.
Phosphate (HPO42−): Major ICF anion; important for ATP, nucleic acids, and buffering.
Causes and Consequences of Electrolyte Imbalances
Electrolyte imbalances can have serious physiological effects. The following table summarizes key abnormalities:
Ion | Abnormality | Possible Causes | Consequences |
|---|---|---|---|
Sodium | Hypernatremia (>145 mEq/L) | Dehydration, excess IV NaCl | Thirst, CNS dehydration, confusion, twitching, convulsions |
Sodium | Hyponatremia (<135 mEq/L) | Solute loss, water retention, diuretics, renal disease, excess ADH | Brain swelling, confusion, coma, circulatory shock |
Potassium | Hyperkalemia (>5.5 mEq/L) | Renal failure, burns, tissue injury | Nausea, arrhythmias, muscle weakness, paralysis |
Potassium | Hypokalemia (<3.5 mEq/L) | GI loss, diuretics, starvation | Arrhythmias, muscle weakness, confusion |
Calcium | Hypercalcemia (>5.2 mEq/L) | Hyperparathyroidism, vitamin D excess | Arrhythmias, muscle weakness, confusion, kidney stones |
Calcium | Hypocalcemia (<4.5 mEq/L) | Hypoparathyroidism, vitamin D deficiency | Tetany, convulsions, fractures |
Magnesium | Hypermagnesemia (>2.2 mEq/L) | Renal failure, antacids | Lethargy, coma, cardiac arrest |
Magnesium | Hypomagnesemia (<1.4 mEq/L) | Alcohol use disorder, diarrhea | Tremors, tetany, convulsions |
Regulation of Sodium Balance
Sodium balance is tightly linked to blood pressure and volume regulation, primarily through hormonal mechanisms.
Aldosterone: Increases Na+ reabsorption (and K+ secretion) in the kidneys, increasing ECF volume and blood pressure.
Renin-Angiotensin-Aldosterone System (RAAS): Activated by low blood pressure/volume, leading to aldosterone release.
Atrial Natriuretic Peptide (ANP): Released by atrial cells in response to high blood pressure; inhibits ADH, renin, and aldosterone, promoting Na+ and water excretion.


Regulation of Potassium Balance
Potassium balance is critical for cell function, especially in excitable tissues like nerves and muscles.
High ECF K+ (hyperkalemia): Depolarizes cells, increasing excitability but can lead to reduced responsiveness and arrhythmias.
Low ECF K+ (hypokalemia): Hyperpolarizes cells, reducing excitability.
Regulation: Kidneys adjust K+ secretion in response to plasma concentration; aldosterone increases K+ secretion.
Regulation of Calcium and Phosphate Balance
Calcium and phosphate levels are regulated mainly by parathyroid hormone (PTH).
PTH Actions:
Stimulates osteoclasts to release Ca2+ and PO43− from bone.
Increases Ca2+ reabsorption and decreases PO43− reabsorption in kidneys.
Activates vitamin D, increasing intestinal absorption of Ca2+.
Clinical Importance: Hypocalcemia increases neuromuscular excitability (tetany); hypercalcemia inhibits neurons and muscle cells (arrhythmias).

Acid-Base Balance
pH and Acid-Base Disorders
Acid-base balance is essential for normal cellular function. The body maintains arterial blood pH around 7.4 (normal range: 7.35–7.45).
Acidosis: Arterial pH < 7.35
Alkalosis: Arterial pH > 7.45
Major Regulatory Mechanisms:
Chemical buffer systems (immediate)
Respiratory regulation (minutes)
Renal regulation (hours to days)
Chemical Buffer Systems
Buffers resist changes in pH by binding or releasing H+. Major buffer systems include:
Bicarbonate Buffer System: Main ECF buffer; involves H2CO3 (weak acid) and HCO3− (weak base).
Phosphate Buffer System: Important in urine and ICF; involves H2PO4− and HPO42−.
Protein Buffer System: Most important in ICF; amino acid side chains act as weak acids or bases.
Respiratory Regulation of Acid-Base Balance
The respiratory system regulates pH by controlling CO2 exhalation, which is in equilibrium with carbonic acid in the blood:
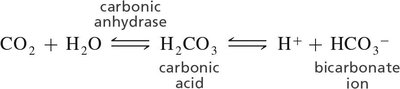
Increased CO2 (hypoventilation) leads to acidosis; decreased CO2 (hyperventilation) leads to alkalosis.
Renal Regulation of Acid-Base Balance
The kidneys provide the most potent acid-base regulation by excreting or reabsorbing H+ and HCO3− as needed.
Conserving or generating new HCO3− is equivalent to losing H+.
Excreting HCO3− is equivalent to gaining H+.
Acid-Base Imbalances
Acid-base disorders are classified as respiratory or metabolic, depending on the primary cause:
Respiratory Acidosis: High PCO2 (>45 mm Hg), low pH; due to hypoventilation.
Respiratory Alkalosis: Low PCO2 (<35 mm Hg), high pH; due to hyperventilation.
Metabolic Acidosis: Low HCO3− (<22 mEq/L), low pH; causes include diarrhea, renal failure, diabetes, starvation, alcohol ingestion.
Metabolic Alkalosis: High HCO3− (>26 mEq/L), high pH; causes include vomiting, diuretics, antacid overuse, excess aldosterone.
Compensation Mechanisms
Respiratory Compensation: Lungs adjust ventilation to correct metabolic pH imbalances.
Renal Compensation: Kidneys adjust HCO3− reabsorption/secretion to correct respiratory pH imbalances.
Effects of Severe pH Imbalances
Blood pH < 6.8: CNS depression, coma, death.
Blood pH > 7.8: Overexcitation of nervous system, tetany, convulsions, death from respiratory arrest.
Additional info: These notes provide a comprehensive overview of fluid, electrolyte, and acid-base balance, integrating textbook content with logical academic context for ANP college students.
