Back
BackFunctional Anatomy and Physiology of the Respiratory System: Chapter 21 Mastery Review
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Dynamic Pipeline: Overview of the Respiratory System
The respiratory system is essential for gas exchange, supporting cellular metabolism by delivering oxygen and removing carbon dioxide. Its structure and function are tightly integrated to maintain homeostasis and support life.
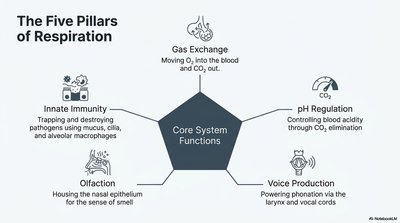
The Five Pillars of Respiration
Core System Functions
The respiratory system performs several critical functions beyond gas exchange, each contributing to overall health and homeostasis.
Gas Exchange: Transfers O2 into the blood and removes CO2.
pH Regulation: Maintains blood acidity by controlling CO2 elimination.
Voice Production: Enables phonation via the larynx and vocal cords.
Olfaction: Houses the nasal epithelium for the sense of smell.
Innate Immunity: Traps and destroys pathogens using mucus, cilia, and alveolar macrophages.
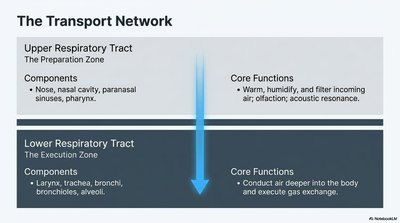
The Transport Network
Upper and Lower Respiratory Tracts
The respiratory tract is divided into upper and lower regions, each with specialized structures and functions.
Region | Components | Core Functions |
|---|---|---|
Upper Respiratory Tract (Preparation Zone) | Nose, nasal cavity, paranasal sinuses, pharynx | Warm, humidify, and filter incoming air; olfaction; acoustic resonance |
Lower Respiratory Tract (Execution Zone) | Larynx, trachea, bronchi, bronchioles, alveoli | Conduct air deeper into the body and execute gas exchange |
The Gateways
Entry Structures and Airflow Pathways
Air enters the respiratory system through specialized structures that filter, warm, and humidify it before reaching the lungs.
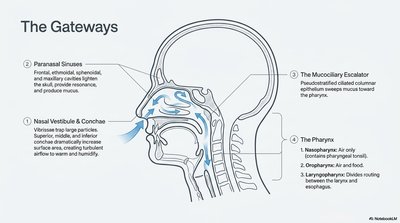
Paranasal Sinuses: Frontal, ethmoidal, sphenoidal, and maxillary cavities lighten the skull, provide resonance, and produce mucus.
Nasal Vestibule & Conchae: Vibrissae trap large particles; conchae increase surface area, enhancing air conditioning.
The Mucociliary Escalator: Pseudostratified ciliated columnar epithelium sweeps mucus toward the pharynx.
The Pharynx: Divided into nasopharynx (air only), oropharynx (air and food), and laryngopharynx (divides routing between larynx and esophagus).
The Voice Box & The Windpipe
Larynx and Trachea
The larynx and trachea serve as critical passageways for air, protect the lower respiratory tract, and enable voice production.
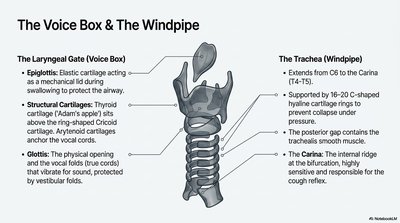
Laryngeal Gate (Voice Box):
Epiglottis: Elastic cartilage acting as a mechanical lid during swallowing.
Structural Cartilages: Thyroid (Adam's apple), cricoid, arytenoid (anchors vocal cords).
Glottis: Opening and vocal folds (true cords) that vibrate for sound, protected by vestibular folds.
Trachea (Windpipe):
Extends from C6 to the carina (T4–T5).
Supported by 16–20 C-shaped hyaline cartilage rings.
Posterior gap contains trachealis smooth muscle.
Carina: Internal ridge at the bifurcation, highly sensitive for the cough reflex.
The Conducting Tree
Bronchial Branching and Zones
The bronchial tree divides air into progressively smaller passages, culminating in the alveoli where gas exchange occurs.
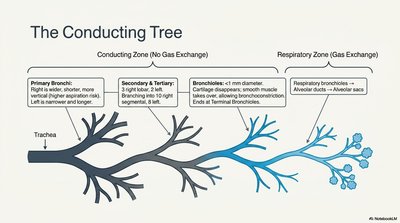
Conducting Zone (No Gas Exchange):
Primary Bronchi: Right is wider, shorter, more vertical; left is narrower and longer.
Secondary & Tertiary Bronchi: 3 right lobar, 2 left; further branching to 10 right and 8 left segments.
Bronchioles: <1 mm diameter, no cartilage, smooth muscle allows constriction/dilation.
Respiratory Zone (Gas Exchange):
Respiratory Bronchioles: Lead to alveolar ducts and alveolar sacs.
The Interface
The Respiratory Membrane and Alveoli
The respiratory membrane is the site of gas exchange, consisting of three layers and specialized cells.
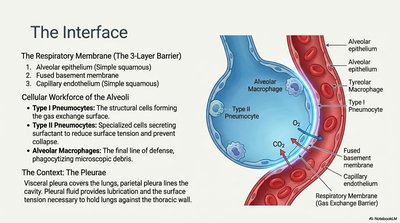
Respiratory Membrane (3-Layer Barrier):
Alveolar epithelium (simple squamous)
Fused basement membrane
Capillary endothelium (simple squamous)
Cellular Workforce of the Alveoli:
Type I Pneumocytes: Form the gas exchange surface.
Type II Pneumocytes: Secrete surfactant to reduce surface tension and prevent collapse.
Alveolar Macrophages: Phagocytose debris and pathogens.
The Pleurae: Visceral pleura covers lungs; parietal pleura lines the cavity. Pleural fluid reduces friction and surface tension.
The Mechanics of Breath
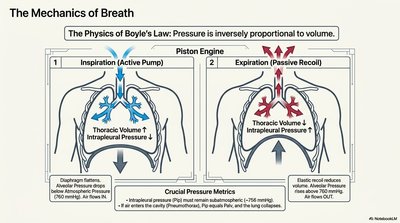
Boyle's Law and Pulmonary Ventilation
Breathing is governed by Boyle's Law, which states that pressure is inversely proportional to volume. Inspiration is active, while expiration is passive.
Inspiration (Active Pump): Diaphragm contracts, thoracic volume increases, intrapleural pressure drops, air flows in.
Expiration (Passive Recoil): Elastic recoil reduces thoracic volume, pressure rises, air flows out.
Key Equation:
Measuring the Breath
Lung Volumes and Ventilation Efficiency
Lung function is assessed by measuring various volumes and capacities, which reflect the efficiency of ventilation.
Tidal Volume (TV): ~500 mL (normal breath)
Inspiratory Reserve Volume (IRV): ~3000 mL
Expiratory Reserve Volume (ERV): ~1100 mL
Residual Volume (RV): ~1200 mL
Vital Capacity (VC): ~4600 mL
Total Lung Capacity (TLC): ~5800 mL
Minute Ventilation: (≈6 L/min)
Alveolar Ventilation: (≈4.2 L/min)

The Symmetrical Exchange
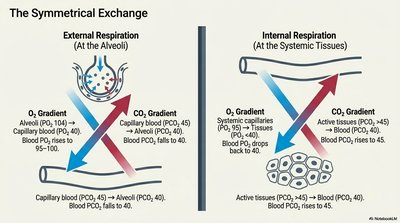
External and Internal Respiration
Gas exchange occurs at two main sites: the alveoli (external respiration) and systemic tissues (internal respiration), driven by partial pressure gradients.
External Respiration: O2 moves from alveoli (PO2 ≈ 104 mmHg) to blood (PO2 ≈ 40 mmHg); CO2 moves from blood (PCO2 ≈ 45 mmHg) to alveoli (PCO2 ≈ 40 mmHg).
Internal Respiration: O2 moves from blood (PO2 ≈ 95 mmHg) to tissues (PO2 < 40 mmHg); CO2 moves from tissues (PCO2 > 45 mmHg) to blood (PCO2 ≈ 40 mmHg).
The Oxygen Courier
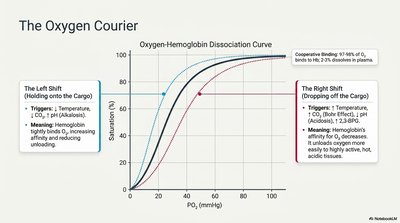
Oxygen-Hemoglobin Dissociation Curve
Hemoglobin's affinity for oxygen changes with physiological conditions, affecting oxygen loading and unloading.
Left Shift: Increased affinity (low temperature, low CO2, alkalosis, low 2,3-BPG); hemoglobin holds onto O2.
Right Shift: Decreased affinity (high temperature, high CO2, acidosis, high 2,3-BPG); hemoglobin releases O2 more readily.
The Carbon Dioxide Return
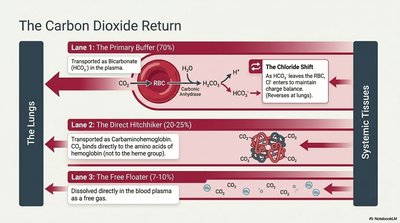
CO2 Transport Mechanisms
Carbon dioxide is transported from tissues to lungs via three main mechanisms:
Transport Lane | Mechanism | Percentage |
|---|---|---|
Primary Buffer | As bicarbonate (HCO3-) in plasma | ~70% |
Direct Hitchhiker | As carbaminohemoglobin (bound to hemoglobin) | ~20–25% |
Free Floater | Dissolved in plasma as free CO2 | ~7–10% |
Chloride Shift: Exchange of HCO3- and Cl- across the RBC membrane to maintain charge balance.
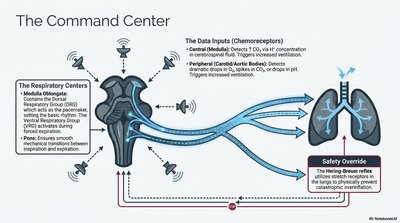
The Command Center
Neural Control of Respiration
Breathing is regulated by respiratory centers in the brainstem, which respond to chemical and mechanical signals.
Medullary Centers: Dorsal and ventral respiratory groups set the basic rhythm.
Pontine Centers: Fine-tune the rhythm and coordinate transitions.
Chemoreceptors: Detect changes in CO2, O2, and pH.
Hering-Breuer Reflex: Prevents overinflation of the lungs.
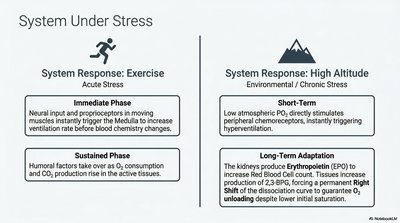
System Under Stress
Adaptations to Exercise and High Altitude
The respiratory system adapts to acute and chronic stressors to maintain oxygen delivery and CO2 removal.
Exercise (Acute Stress):
Immediate Phase: Neural input increases ventilation rate.
Sustained Phase: Humoral factors (CO2, O2) adjust breathing to match metabolic demand.
High Altitude (Chronic Stress):
Short-Term: Low atmospheric O2 stimulates hyperventilation.
Long-Term: Kidneys produce erythropoietin (EPO) to increase RBC count; tissues increase 2,3-BPG to facilitate O2 unloading.
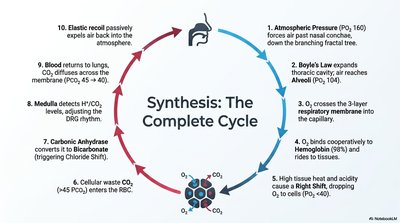
Synthesis: The Complete Cycle
Summary of the Respiratory Cycle
The respiratory cycle integrates atmospheric pressure, gas laws, membrane diffusion, hemoglobin binding, and neural control to sustain life.
Atmospheric pressure drives air into the nasal cavity.
Boyle's Law expands thoracic cavity, air reaches alveoli.
O2 crosses the respiratory membrane into capillaries.
O2 binds to hemoglobin, is delivered to tissues.
High tissue CO2 and acidity cause O2 unloading (Right Shift).
Cellular waste CO2 enters RBCs.
Carbonic anhydrase converts CO2 to bicarbonate (HCO3-).
Medulla detects CO2/H+ levels, adjusts breathing.
Blood returns CO2 to lungs for exhalation.
Elastic recoil expels air back into the atmosphere.