 Back
BackHeart Failure: Pathophysiology, Diagnosis, and Special Syndromes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Heart Failure: Overview
Definition and General Concepts
Heart failure is a clinical syndrome in which the heart is unable to pump sufficient blood to meet the metabolic needs of the body. It results from structural or functional cardiac disorders that impair the ventricle's ability to fill with or eject blood.
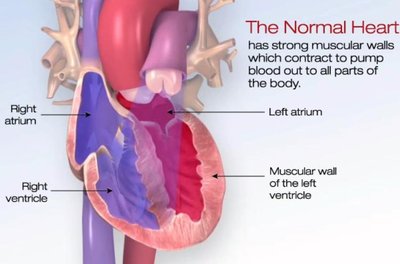
Normal Heart Function: The heart's muscular walls contract to pump blood efficiently throughout the body.
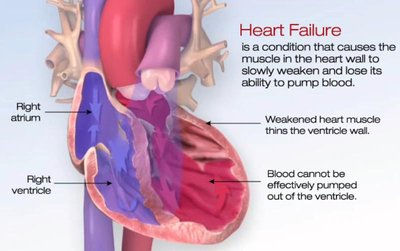
Heart Failure: The heart muscle weakens, leading to reduced pumping ability and symptoms such as dyspnea, fatigue, and edema.
Heart Failure with Reduced Ejection Fraction (HFrEF)
Ejection Fraction (EF) and Its Significance
Ejection Fraction (EF) is a key measurement in assessing systolic heart function. It represents the percentage of blood ejected from the ventricle with each contraction.
Normal EF: 50–70%
Reduced EF: <50% (indicative of systolic dysfunction)
Formula:

Pathophysiology of HFrEF
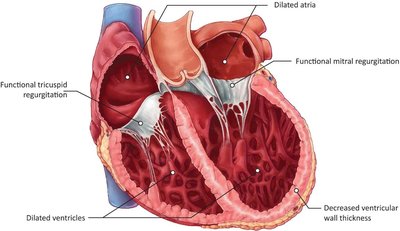
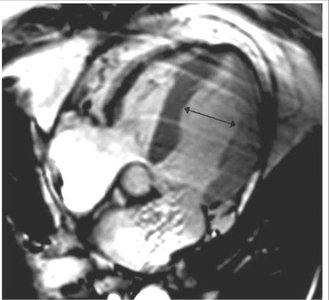
HFrEF is characterized by impaired ventricular contractility, leading to incomplete ejection of blood, increased end-diastolic volume, and ventricular dilation.
Myocardial Injury: Causes decreased contractility and incomplete ejection.
Volume Overload: Increased end-diastolic volume leads to dilation and thinning of the ventricular wall.
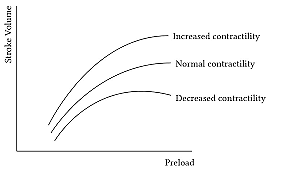
Frank-Starling Law: Increased filling stretches myocytes, enhancing contraction up to a physiological limit.
Etiologies of Dilated Cardiomyopathy (DCM)
DCM is a common cause of HFrEF and can result from various genetic, infectious, toxic, endocrine, or peripartum factors.
Genetic: Mutations in titin, troponin T, phospholamban, dystrophin
Infectious: Myocarditis
Toxic: Alcohol, cobalt, lead
Endocrine: Diabetes, thyroid dysfunction
Peripartum: Pregnancy and postpartum period
Maladaptive Remodeling and Neurohormonal Activation
Initially, neurohormonal activation (e.g., sympathetic nervous system, renin-angiotensin-aldosterone system) compensates for reduced cardiac output. Chronically, these pathways promote maladaptive remodeling and worsen heart failure.
β-adrenergic Receptors: Chronic stimulation leads to receptor downregulation and decreased cAMP-PKA signaling.
GRK2: Phosphorylates β-receptors, promoting internalization and degradation.
Result: Reduced contractility and further decline in cardiac function.

Diagnosis of HFrEF
Diagnosis is based on clinical symptoms, imaging, and laboratory findings.
Symptoms: Dyspnea, fatigue, peripheral edema
Echocardiography: Measures EF, chamber size, and wall motion
Biomarkers: Natriuretic peptides (BNP, NT-proBNP)
ECG and Chest X-ray: Assess for arrhythmias and pulmonary congestion
Treatment of HFrEF
Treatment aims to address the underlying cause, block maladaptive neurohormonal pathways, and relieve symptoms.
Underlying Causes: Treat ischemia, hypertension, valvular disease
Neurohormonal Blockade: β-blockers, ACE inhibitors, ARBs
Diuretics: For volume control and symptom relief
Advanced Therapies: Devices (e.g., ICD, CRT), heart transplant in selected patients
Takotsubo Cardiomyopathy (Stress-Induced Cardiomyopathy)
Definition and Clinical Features
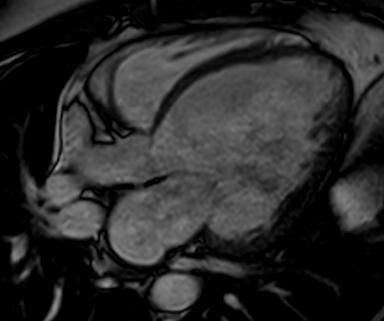
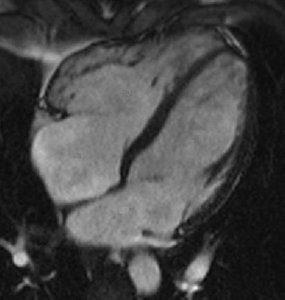
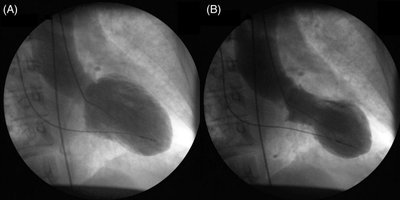
Takotsubo cardiomyopathy is an acute, reversible cardiac syndrome often triggered by emotional or physical stress. It is more prevalent in women and is characterized by transient left ventricular dysfunction, typically involving the apex (apical ballooning).
Symptoms: Chest pain, dyspnea, ECG changes mimicking myocardial infarction
Imaging: Apical akinesis with preserved basal contraction
Pathophysiology
The syndrome is thought to result from a catecholamine surge, leading to differential stimulation of β-adrenergic receptors in the heart. High concentrations of β2-adrenergic receptors in the apex may cause regional myocardial stunning.
β1-adrenergic Receptors: Increase contractility
β2-adrenergic Receptors: At high catecholamine levels, may decrease contractility (especially in the apex)
Emotional Triggers and Epidemiology
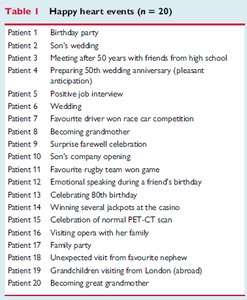
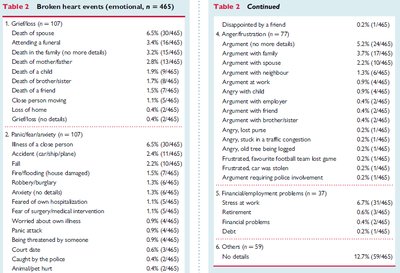
Takotsubo cardiomyopathy can be triggered by both negative ("broken heart") and positive ("happy heart") emotional events. Epidemiological studies have catalogued a wide range of triggers.
Happy Heart Events (n = 20) |
|---|
Birthday party, Son's wedding, Meeting friends, Wedding, Becoming grandmother, Positive job interview, etc. |
Broken Heart Events (n = 465) |
|---|
Grief/loss, Death of spouse, Attending a funeral, Illness, Financial/employment problems, Interpersonal conflict, etc. |
Clinical Case Example
Takotsubo syndrome can be triggered by acute emotional stress, such as witnessing a missed penalty kick in a soccer match, leading to transient cardiac dysfunction in susceptible individuals.

Summary Table: Heart Failure vs. Takotsubo Cardiomyopathy
Feature | HFrEF | Takotsubo Cardiomyopathy |
|---|---|---|
Etiology | Chronic myocardial injury, DCM, ischemia | Acute emotional/physical stress |
Pathophysiology | Ventricular dilation, reduced contractility | Transient apical ballooning, catecholamine surge |
Clinical Course | Chronic, progressive | Acute, reversible |
Imaging | Dilated chambers, thin walls | Apical akinesis, ballooning |
Key Learning Objectives
Define heart failure and ejection fraction.
Explain the pathophysiology of HFrEF, including volume overload and ventricular dilation.
Identify major etiologies of dilated cardiomyopathy.
Describe neurohormonal activation and its role in maladaptive remodeling.
Describe the hallmark features and mechanism of Takotsubo cardiomyopathy.
