 Back
BackHigher Mental Functions, Brain Protection, and Spinal Cord: Structure and Function
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Higher Mental Functions
Language
Language is a complex higher mental function involving several regions of the cerebral cortex, primarily in the left hemisphere. The Broca’s area is responsible for speech production, while the Wernicke’s area is essential for understanding spoken and written language. Damage to these areas results in distinct language deficits: Broca’s aphasia impairs speech production but not comprehension, whereas Wernicke’s aphasia allows fluent but nonsensical speech with poor comprehension. The right hemisphere contains corresponding regions that process nonverbal aspects of communication, such as tone and emotion.

Memory
Memory is the process of storing and retrieving information. There are several types of memory:
Declarative (fact) memory: Facts such as names, faces, words, and dates.
Procedural (skills) memory: Skills like playing the piano.
Motor memory: Motor skills such as riding a bike.
Emotional memory: Emotional responses linked to experiences.
Declarative memory is stored in two stages:
Short-term memory (STM): Temporary storage, limited to 7–8 items.
Long-term memory (LTM): Virtually limitless capacity.
Factors influencing transfer from STM to LTM include emotional state, rehearsal, association, and automatic memory. Memory consolidation involves the hippocampus, temporal cortex, thalamus, and prefrontal cortex.

Clinical Aspects of Memory
Anterograde amnesia: Inability to form new memories; old memories remain intact.
Retrograde amnesia: Loss of memories formed in the past.
Consciousness
Consciousness encompasses awareness of sensations, voluntary movements, and higher mental processing. It exists on a continuum from alertness to coma. Loss of consciousness (except during sleep) indicates impaired brain function and can result from fainting, coma, or brain death.
Alertness: Highest state of consciousness.
Drowsiness: Mildly reduced awareness.
Stupor: Markedly reduced responsiveness.
Coma: Complete unresponsiveness.
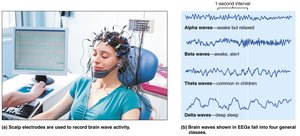
Brain Waves and the EEG
Brain waves are patterns of neuronal electrical activity recorded by an electroencephalogram (EEG). EEGs are used to diagnose epilepsy, sleep disorders, and brain death. Brain waves are classified by frequency (Hz):
Alpha waves (8–13 Hz): Indicate a relaxed, awake state.
Beta waves (14–30 Hz): Present during mental activity and alertness.
Theta waves (4–7 Hz): Common in children, abnormal in awake adults.
Delta waves (<4 Hz): Seen in deep sleep or brain damage in awake adults.
Clinical Aspects: Epilepsy
Epileptic seizures: Sudden electrical discharges in the brain causing loss of consciousness and convulsions.
Absence seizures: Brief, mild episodes, often in children.
Tonic-clonic seizures: Severe, with loss of consciousness and convulsions.
Treatment includes anticonvulsants and, in some cases, nerve stimulators.
Sleep and Sleep-Wake Cycles
Sleep is a state of partial unconsciousness with two main types:
Non–rapid eye movement (NREM) sleep: Four stages, progressing from light to deep sleep.
Rapid eye movement (REM) sleep: Characterized by dreaming, increased brain activity, and temporary muscle paralysis.
Sleep is regulated by the hypothalamus and follows a circadian rhythm. It is essential for memory consolidation and brain restoration.

Clinical Aspects: Sleep Disorders
Narcolepsy: Sudden sleep attacks due to loss of hypothalamic orexins.
Insomnia: Chronic inability to sleep, often related to stress or lifestyle.
Protection of the Brain
Meninges
The meninges are three connective tissue membranes that protect the CNS, contain cerebrospinal fluid (CSF), and form partitions within the skull:
Dura mater: Outermost, toughest layer; forms dural septa and venous sinuses.
Arachnoid mater: Middle, web-like layer; contains CSF and blood vessels.
Pia mater: Innermost, delicate layer; adheres to brain surface and contains blood vessels.
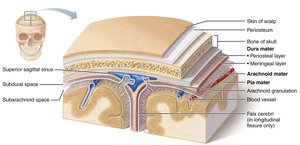
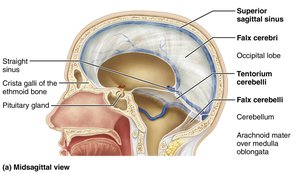
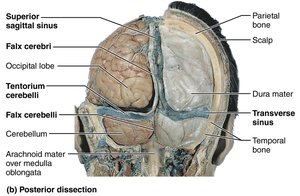
Dural Septa and Sinuses
Dura mater forms partitions (septa) that limit brain movement and house venous sinuses for blood drainage:
Falx cerebri: In the longitudinal fissure.
Falx cerebelli: Along the cerebellum.
Tentorium cerebelli: Over the cerebellum.
Clinical Aspects: Meningitis
Meningitis: Inflammation of the meninges, diagnosed by CSF analysis.
Can lead to encephalitis if it spreads to the brain.
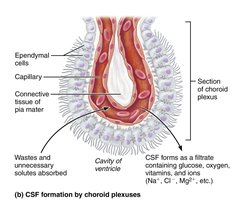
Cerebrospinal Fluid (CSF)
CSF is a clear fluid that cushions the brain, reduces its weight, protects against trauma, and nourishes neural tissue. It is produced by the choroid plexus and circulates through the ventricles and subarachnoid space, eventually being reabsorbed into the venous blood.
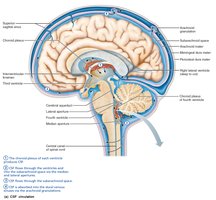
Clinical Aspects: Hydrocephalus
Hydrocephalus: Blocked CSF drainage increases intracranial pressure, causing head enlargement in infants and brain damage in adults. Treated by shunting CSF to another body cavity.
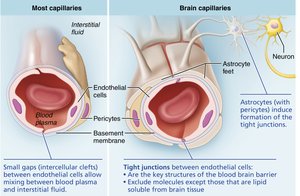
Blood Brain Barrier
The blood brain barrier protects the brain from harmful substances in the blood while allowing essential nutrients to pass. It consists of tight junctions between endothelial cells, a thick basement membrane, and astrocyte feet. Lipid-soluble substances pass freely, while others require specific transport mechanisms.
Brain Injuries and Disorders
Traumatic Brain Injuries
Concussion: Temporary functional disturbance.
Contusion: Permanent brain damage.
Hemorrhage: Bleeding increases intracranial pressure, potentially fatal.
Cerebral edema: Swelling due to injury.
Cerebrovascular Accidents (Strokes)
Ischemia: Blocked blood flow causes tissue death.
Hemiplegia: Paralysis on one side of the body.
Transient ischemic attacks (TIAs): Temporary, reversible episodes.
Tissue plasminogen activator (TPA): Approved treatment for stroke.
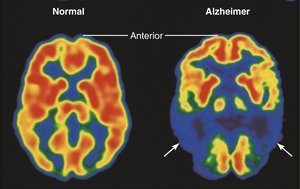
Degenerative Brain Disorders
Alzheimer’s disease: Progressive dementia due to protein misfolding, beta-amyloid plaques, and neurofibrillary tangles. Treated with drugs targeting neurotransmitter breakdown and toxic protein accumulation.
Parkinson’s disease: Degeneration of dopamine neurons causes tremors and motor deficits. Treated with L-dopa and deep brain stimulation.
Huntington’s disease: Hereditary disorder with wild movements and mental decline due to huntingtin protein accumulation.
Spinal Cord: Structure and Function
Gross Anatomy and Protection
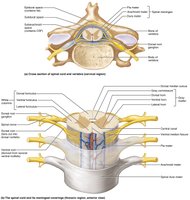
The spinal cord is protected by vertebrae, meninges, and CSF. It begins at the foramen magnum and ends at the conus medullaris. The filum terminale anchors the cord, and denticulate ligaments secure it laterally. Spinal nerves attach by paired roots, and the cauda equina is a bundle of nerve roots at the lower end.


Spinal Cord Cross-Sectional Anatomy
The spinal cord has central gray matter (neuronal cell bodies) and peripheral white matter (myelinated axons). The gray matter is organized into dorsal, ventral, and lateral horns, and the white matter is divided into dorsal, lateral, and ventral columns (funiculi). Spinal nerves are formed by the fusion of dorsal (sensory) and ventral (motor) roots.

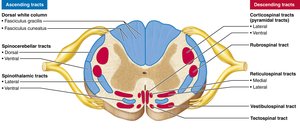
Major Ascending and Descending Tracts
Ascending (sensory) tracts carry information to the brain, while descending (motor) tracts carry commands from the brain to the body. Major ascending pathways include the dorsal column–medial lemniscal, spinothalamic, and spinocerebellar tracts. Major descending pathways include direct (pyramidal) and indirect (extrapyramidal) tracts.


Spinal Cord Trauma and Disorders
Paresthesias: Sensory loss due to dorsal root damage.
Paralysis: Motor loss due to ventral root damage; can be flaccid or spastic.
Transection: Complete severing causes loss of function below the injury (paraplegia or quadriplegia).
Poliomyelitis: Viral destruction of ventral horn neurons.
Amyotrophic lateral sclerosis (ALS): Degeneration of motor neurons, leading to muscle weakness and death.
Neuronal Pathways
Ascending Pathways
Ascending pathways conduct sensory information through a chain of three neurons (first-order, second-order, third-order) to the brain. Main pathways include:
Dorsal column–medial lemniscal: Discriminative touch and vibration.
Spinothalamic: Pain, temperature, coarse touch, and pressure.
Spinocerebellar: Muscle and tendon stretch for coordination.
Descending Pathways
Descending pathways deliver motor commands from the brain to the spinal cord. They include:
Direct (pyramidal) pathways: Fast, skilled movements.
Indirect pathways: Balance, posture, and coarse movements.
Developmental Aspects of the CNS
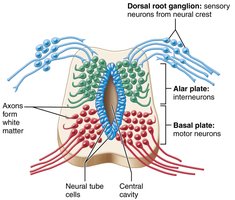
Neural Tube Formation
The CNS develops from the neural tube, which forms from the ectoderm in the embryo. The neural tube differentiates into the brain and spinal cord, with neural crest cells forming peripheral structures.

Clinical Aspects: Developmental Disorders
Cerebral palsy: Neuromuscular disability from brain damage at birth.
Anencephaly: Failure of the cerebrum and brain stem to develop.
Spina bifida: Incomplete formation of vertebral arches, often due to folic acid deficiency.
