Back
Back(Exam) Integrated Physiology of the Muscular and Cardiovascular Systems: Synthesis Guide
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Engine & The Fuel: Integrated Physiology of the Muscular and Cardiovascular Systems
Overview
This module synthesizes the physiology of the muscular and cardiovascular systems, focusing on their interdependence for movement, energy, and homeostasis. It integrates concepts from muscle structure and function, blood composition, and clinical applications relevant to ANP college courses (Chapters 9, 17, and related synthesis topics).
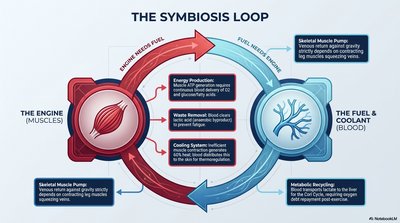
The Symbiosis Loop: Muscles and Blood
Muscle-Blood Interdependence
The muscular system (engine) and cardiovascular system (fuel/coolant) operate in a symbiotic loop, each supporting the other's function during activity.
Muscles (Engine): Require oxygen and nutrients for ATP production, generate waste (CO2, heat), and rely on blood for cooling and waste removal.
Blood (Fuel & Coolant): Delivers oxygen and nutrients, removes metabolic waste, and recycles metabolites (e.g., lactate).
Skeletal Muscle Pump: Muscle contractions assist venous return by squeezing veins, enhancing circulation during exercise.
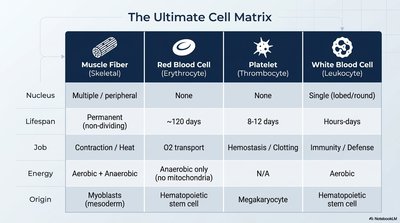
The Ultimate Cell Matrix
Key Cell Types in Muscle and Blood
Muscle fibers, red blood cells, platelets, and white blood cells each have specialized structures and functions essential for integrated physiology.
Muscle Fiber (Skeletal) | Red Blood Cell (Erythrocyte) | Platelet (Thrombocyte) | White Blood Cell (Leukocyte) | |
|---|---|---|---|---|
Nucleus | Multiple / peripheral | None | None | Single (lobed/round) |
Lifespan | Permanent (non-dividing) | ~120 days | 8-12 days | Hours-days |
Job | Contraction / Heat | O2 transport | Hemostasis / Clotting | Immunity / Defense |
Energy | Aerobic + Anaerobic | Anaerobic only (no mitochondria) | N/A | Aerobic |
Origin | Myoblasts (mesoderm) | Hematopoietic stem cell | Megakaryocyte | Hematopoietic stem cell |
Muscle Architecture & Contraction Mechanics
Muscle Structure
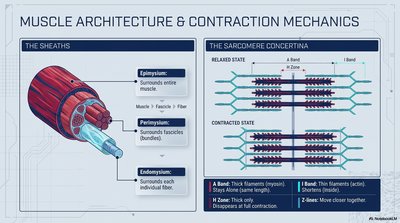
Muscles are organized into hierarchical sheaths and contract via the sliding filament mechanism within sarcomeres.
Epimysium: Surrounds entire muscle.
Perimysium: Surrounds fascicles (bundles).
Endomysium: Surrounds each individual fiber.
Sarcomere Contraction
Relaxed State: A band (thick filaments) and I band (thin filaments) visible; Z lines farther apart.
Contracted State: I band shortens, Z lines move closer, A band remains constant.
The Spark: Neuromuscular Junction (NMJ) Flow & Muscle Levers
NMJ Flow
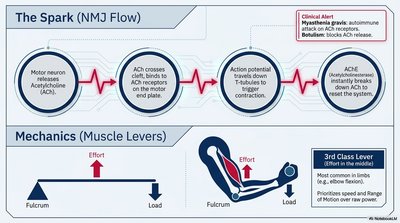
Muscle contraction is initiated by nerve impulses at the neuromuscular junction (NMJ):
Motor neuron releases acetylcholine (ACh).
ACh binds to receptors on the muscle end plate.
Action potential travels down T-tubules, triggering contraction.
Acetylcholinesterase (AChE) breaks down ACh to reset the system.
Clinical Alert: Myasthenia gravis (autoimmune attack on ACh receptors) and botulism (blocks ACh release) disrupt NMJ function.
Muscle Levers
3rd Class Lever: Most common in limbs; effort is between fulcrum and load, maximizing speed and range of motion.
The Cross-Bridge Cycle
Steps of Muscle Contraction
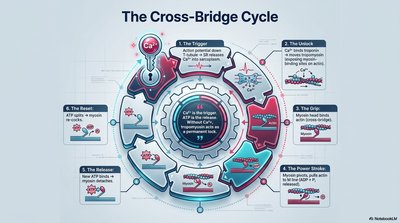
The cross-bridge cycle describes the molecular events of muscle contraction:
The Trigger: Ca2+ binds to troponin, exposing myosin-binding sites on actin.
The Unlock: Myosin heads bind to actin, forming cross-bridges.
The Grip: Myosin head pivots, pulling actin (power stroke).
The Power Stroke: ADP and Pi are released.
The Release: ATP binds to myosin, causing detachment from actin.
The Reset: ATP hydrolysis re-cocks the myosin head.
Fiber Types & Energy Systems
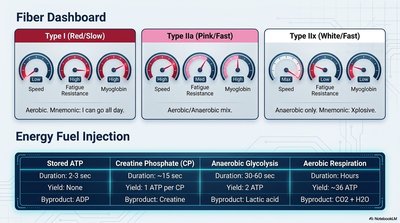
Muscle Fiber Types
Type I (Red/Slow): High endurance, aerobic, high myoglobin.
Type IIa (Pink/Fast): Intermediate, aerobic/anaerobic mix.
Type IIx (White/Fast): Explosive, anaerobic, low myoglobin.
Energy Pathways
System | Duration | Yield | Byproduct |
|---|---|---|---|
Stored ATP | 2-3 sec | 1 ATP | ADP |
Creatine Phosphate (CP) | ~15 sec | 1 ATP per CP | Creatine |
Anaerobic Glycolysis | 30-60 sec | 2 ATP | Lactic acid |
Aerobic Respiration | Hours | ~36 ATP | CO2 + H2O |
Whole Blood Composition
Blood Components
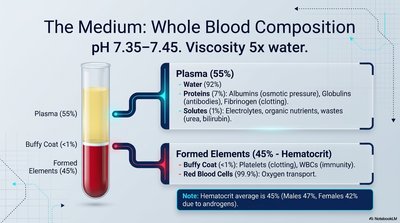
Blood is a complex fluid with a pH of 7.35–7.45 and viscosity five times that of water.
Plasma (55%): Mostly water (92%), proteins (albumins, globulins, fibrinogen), and solutes (electrolytes, nutrients, wastes).
Formed Elements (45%): Red blood cells (O2 transport), white blood cells (immunity), platelets (clotting).
Hematocrit: Percentage of RBCs in blood (average 45%).
Red Blood Cells & Hemoglobin
Structure and Function
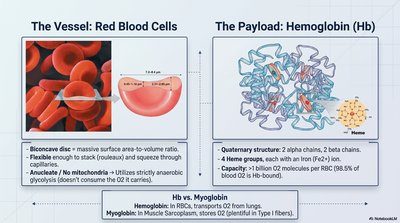
Red Blood Cells (RBCs): Biconcave discs, flexible, anucleate, no mitochondria (rely on anaerobic glycolysis).
Hemoglobin (Hb): Quaternary protein with 4 heme groups (each binds 1 O2), transports O2 from lungs to tissues.
Myoglobin: Found in muscle, stores O2 for rapid use.
Erythropoiesis & RBC Recycling
Production and Breakdown
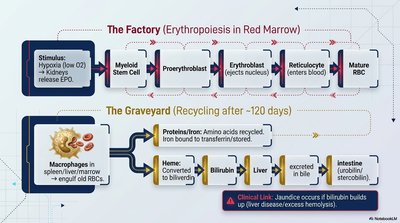
Erythropoiesis: Stimulated by hypoxia (low O2), kidneys release erythropoietin (EPO), promoting RBC production in red marrow.
RBC Recycling: After ~120 days, macrophages break down old RBCs; proteins and iron are recycled, heme is converted to bilirubin (excreted in bile).
Clinical Link: Jaundice results from excess bilirubin due to liver dysfunction or excessive hemolysis.
White Blood Cells & Hemostasis
WBC Types and Functions
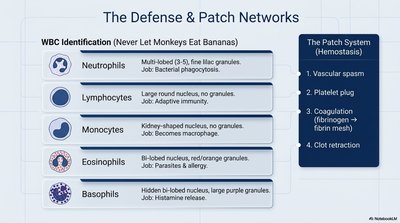
Neutrophils: Phagocytosis of bacteria.
Lymphocytes: Adaptive immunity.
Monocytes: Become macrophages.
Eosinophils: Parasite and allergy defense.
Basophils: Histamine release (inflammation).
Hemostasis (Clotting)
Vascular spasm
Platelet plug formation
Coagulation (fibrin mesh)
Clot retraction
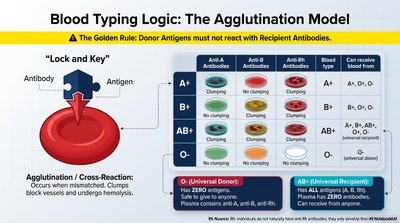
Blood Typing & Agglutination
Blood Groups and Transfusion Logic
Antigens: Surface markers on RBCs (A, B, Rh).
Antibodies: Plasma proteins that react with foreign antigens.
Agglutination: Occurs if donor antigens react with recipient antibodies, causing clumping and hemolysis.
Universal Donor: O- (no antigens).
Universal Recipient: AB+ (no antibodies).
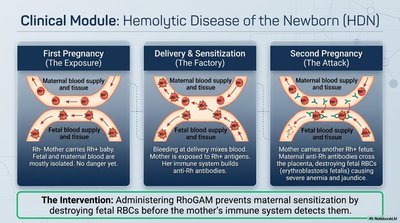
Clinical Module: Hemolytic Disease of the Newborn (HDN)
Pathophysiology and Prevention
First Pregnancy: Rh- mother carries Rh+ fetus; no initial danger.
Delivery/Sensitization: Fetal blood exposure sensitizes mother to Rh antigen.
Second Pregnancy: Maternal anti-Rh antibodies attack fetal RBCs, causing hemolysis and jaundice.
Intervention: RhoGAM prevents sensitization by destroying fetal RBCs before maternal immune response.
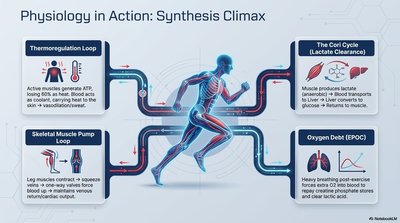
Physiology in Action: Synthesis Climax
Integrated Responses During Exercise
Thermoregulation Loop: Muscles generate heat; blood distributes heat to skin for cooling.
Skeletal Muscle Pump Loop: Muscle contractions enhance venous return, supporting cardiovascular output.
The Cori Cycle: Lactate from muscles is converted to glucose in the liver, clearing acid and recycling energy.
Oxygen Debt (EPOC): Increased respiration post-exercise replenishes O2 and clears lactic acid.
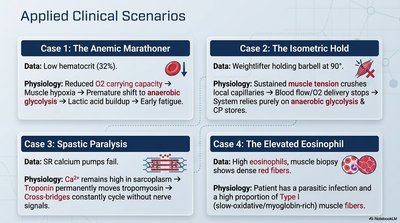
Applied Clinical Scenarios
Examples of Pathophysiology
Case 1: The Anemic Marathoner Low hematocrit reduces O2 carrying capacity, leading to muscle hypoxia, early fatigue, and reliance on anaerobic glycolysis.
Case 2: The Isometric Hold Sustained muscle tension limits blood flow, causing reliance on anaerobic metabolism and rapid fatigue.
Case 3: Spastic Paralysis High Ca2+ in sarcoplasm causes constant cross-bridge cycling, preventing muscle relaxation.
Case 4: The Elevated Eosinophil High eosinophils indicate parasitic infection or allergy; muscle biopsy shows red fibers (Type I, high myoglobin).