 Back
BackPeripheral Nervous System (PNS): Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Peripheral Nervous System (PNS): Overview and Organization
Introduction to the Peripheral Nervous System
The Peripheral Nervous System (PNS) serves as the communication network linking the Central Nervous System (CNS) with the rest of the body and the external environment. It is responsible for detecting sensory stimuli and transmitting this information to the CNS, which processes the input and sends motor commands back through the PNS to effectors such as muscles and glands.
Sensory Input: PNS detects changes in the environment and relays information to the CNS.
Motor Output: CNS sends commands via the PNS to initiate responses in effectors.
Spinal and Cranial Nerves: Both are part of the PNS, even though they attach directly to the spinal cord and brain.
Divisions of the Peripheral Nervous System
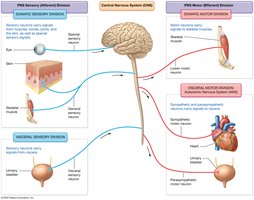
The PNS is divided into sensory (afferent) and motor (efferent) divisions, each with somatic and visceral components.
Sensory (Afferent) Division:
Somatic Sensory Division: Carries signals from skin, muscles, bones, and joints to the CNS.
Visceral Sensory Division: Transmits signals from internal organs (thoracic and abdominopelvic cavities) to the CNS.
Motor (Efferent) Division:
Somatic Motor Division: Sends signals to skeletal muscles for voluntary movement.
Visceral Motor Division (Autonomic Nervous System, ANS): Regulates cardiac and smooth muscle and glands. Subdivided into:
Sympathetic Nervous System: "Fight or Flight" responses.
Parasympathetic Nervous System: "Rest and Digest" activities.
Peripheral Nerves and Associated Ganglia
Structure and Types of Peripheral Nerves
Peripheral nerves are bundles of axons from many neurons, surrounded by connective tissue sheaths. They innervate most body structures and are classified as:
Mixed Nerves: Contain both sensory and motor axons (most common type).
Sensory Nerves: Contain only sensory axons.
Motor Nerves: Primarily motor axons, with some sensory fibers for feedback.
Cranial nerves attach to the brain and innervate the head and neck, while spinal nerves branch from the spinal cord and innervate structures below the neck.
Connective Tissue Sheaths of Nerves
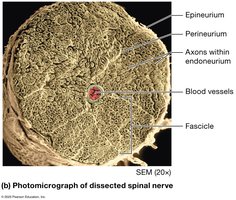
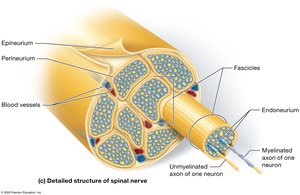
Peripheral nerves are organized into fascicles and surrounded by three connective tissue layers:
Epineurium: Outermost sheath surrounding the entire nerve.
Perineurium: Sheath surrounding each fascicle (bundle of axons).
Endoneurium: Sheath surrounding individual axons.
Functional Overview of the PNS
Sensory and Motor Pathways
Sensory neurons detect stimuli at specialized receptors and transmit signals to the CNS for processing. The CNS interprets these signals and initiates appropriate motor responses, which are relayed back through the PNS to effectors (muscles or glands).
Sensory Pathway: Sensory receptor → Sensory neuron → CNS
Motor Pathway: CNS → Motor neuron → Effector
The Cranial Nerves
Overview and Classification
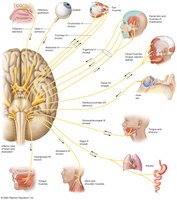
There are twelve pairs of cranial nerves, each with specific sensory, motor, or mixed functions. They are often remembered using mnemonics for their order and function.
Sensory Only: Olfactory (I), Optic (II), Vestibulocochlear (VIII)
Motor Only: Oculomotor (III), Trochlear (IV), Abducens (VI), Accessory (XI), Hypoglossal (XII)
Mixed: Trigeminal (V), Facial (VII), Glossopharyngeal (IX), Vagus (X)
Clinical Correlations
Trigeminal Neuralgia
Trigeminal neuralgia is a chronic pain syndrome affecting one or more branches of the trigeminal nerve, causing brief, intense facial pain. Triggers include chewing, touch, or even a breeze. Treatment may involve anticonvulsant drugs.
Bell’s Palsy
Bell’s palsy is a condition where the facial nerve’s motor root is impaired, leading to facial muscle weakness or paralysis, often with rapid onset. It may affect eye closure, facial expressions, and sometimes taste. Most individuals recover within weeks, sometimes with medication or therapy.
Spinal Nerves and Plexuses
Structure and Distribution
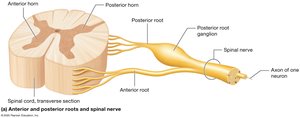
There are 31 pairs of spinal nerves, each splitting into dorsal (posterior) and ventral (anterior) rami. The anterior rami of certain spinal nerves form complex networks called nerve plexuses (cervical, brachial, lumbar, sacral), which innervate limbs and other regions.
Cervical Plexus: Innervates neck, diaphragm (via phrenic nerve).
Brachial Plexus: Innervates upper limb.
Lumbar Plexus: Innervates pelvis and lower limb.
Sacral Plexus: Innervates pelvis, gluteal region, and lower limb (sciatic nerve is the largest).
Sensory Receptors and Sensation
Types and Classification of Sensory Receptors
Sensory receptors convert environmental stimuli into electrical signals (sensory transduction). They are classified by structure, location, and stimulus type:
Encapsulated Nerve Endings: Surrounded by supporting cells (e.g., Meissner corpuscles).
Free Nerve Endings: Lack supporting cells (e.g., nociceptors).
By Location: Exteroceptors (external stimuli), Interoceptors (internal stimuli).
By Stimulus: Mechanoreceptors (touch, pressure), Thermoreceptors (temperature), Chemoreceptors (chemicals), Photoreceptors (light), Nociceptors (pain).
Motor Output and Reflexes
Motor Neurons and Reflex Arcs
Lower motor neurons in the PNS stimulate skeletal muscle contraction. Reflexes are rapid, involuntary responses to stimuli, following a specific neural pathway called a reflex arc:
Sensory receptor
Sensory neuron
Integrating center (CNS)
Motor neuron
Effector (muscle or gland)
Types of Reflexes
Monosynaptic Reflex: Single synapse (e.g., patellar reflex).
Polysynaptic Reflex: Multiple synapses (e.g., withdrawal reflex).
Somatic Reflex: Involves skeletal muscle.
Visceral Reflex: Involves smooth/cardiac muscle or glands.
Clinical Disorders of the PNS
Peripheral Neuropathies
Disorders affecting sensory and motor neurons of the PNS can result in sensory loss, muscle weakness, or paralysis. Examples include:
Lower Motor Neuron Disorders: Injury or disease affecting spinal/cranial nerves or their cell bodies.
Upper Motor Neuron Disorders: Affect CNS pathways, leading to spasticity and abnormal reflexes (e.g., Babinski sign).
Amyotrophic Lateral Sclerosis (ALS): Degeneration of motor neurons, causing progressive muscle weakness and, in some cases, cognitive changes.
