 Back
BackPeripheral Nervous System: Structure, Function, and Cranial Nerves
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Peripheral Nervous System (PNS) Overview
Structural Organization of the Nervous System
The nervous system is divided into the Central Nervous System (CNS) and the Peripheral Nervous System (PNS). The PNS connects the CNS to limbs and organs, serving as a communication relay.
Sensory (afferent) division: Transmits sensory information from receptors to the CNS.
Motor (efferent) division: Transmits commands from the CNS to effector organs.
Somatic nervous system: Controls voluntary movements via skeletal muscles.
Autonomic nervous system (ANS): Regulates involuntary functions (e.g., heart, smooth muscle, glands) and is subdivided into sympathetic and parasympathetic divisions.
Neuronal Structure and Synaptic Transmission
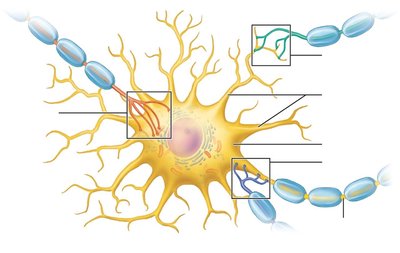
General Structure of a Neuron
Neurons are the functional units of the nervous system, specialized for communication.
Cell body (soma): Contains the nucleus and organelles.
Dendrites: Receive synaptic inputs from other neurons.
Axon: Conducts electrical impulses away from the cell body.
Synapses: Sites of communication between neurons, classified as axodendritic, axosomatic, or axoaxonal.
Synaptic Potentials: Depolarization and Hyperpolarization
Neurons communicate via changes in membrane potential:
Depolarization: Membrane potential becomes less negative (moves toward 0 mV), increasing the likelihood of generating an action potential.
Hyperpolarization: Membrane potential becomes more negative, decreasing the likelihood of an action potential.
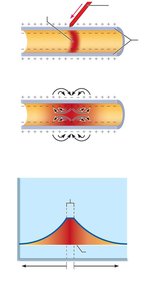
Spread and Decay of Graded Potentials
Graded (synaptic) potentials are local changes in membrane potential that decrease in magnitude with distance from the stimulus site. They are important for short-distance signaling within neurons.
Depolarization spreads via local currents but decays due to leakage across the plasma membrane.
Graded potentials are not regenerated along the membrane.
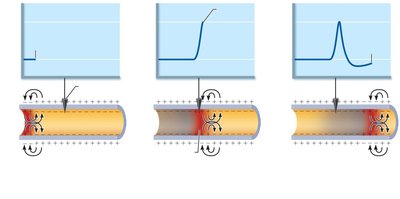
Action Potentials: Propagation and Frequency
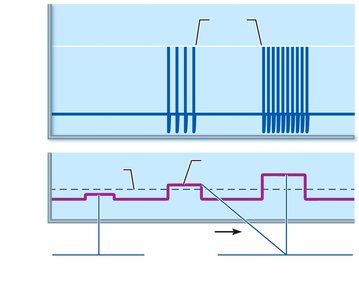
Action potentials (APs) are rapid, long-distance electrical signals generated by neurons when a threshold is reached.
APs are all-or-none events: a stimulus must reach threshold to trigger an AP.
The frequency of APs encodes stimulus strength: stronger stimuli generate more frequent APs.
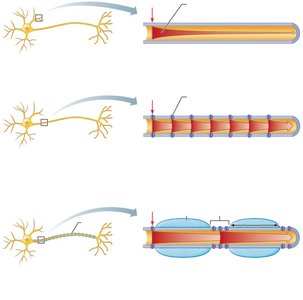
Myelination and Conduction Velocity
Myelination increases the speed of action potential conduction along axons.
Schwann cells (in PNS) wrap around axons, forming a myelin sheath that insulates the axon and allows for saltatory conduction.
In myelinated axons, APs jump from one node of Ranvier to the next, greatly increasing conduction speed.
In nonmyelinated axons, APs propagate more slowly as they must be regenerated at every point along the axon.

Structure and Classification of Nerves
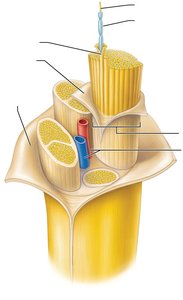
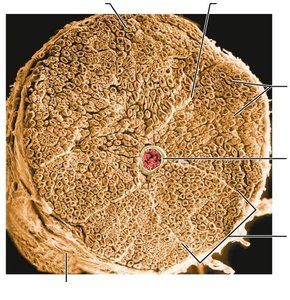
Structure of a Nerve
Nerves are cordlike organs of the PNS, consisting of bundles of myelinated and nonmyelinated axons enclosed by connective tissue layers:
Endoneurium: Surrounds individual axons.
Perineurium: Bundles groups of axons into fascicles.
Epineurium: Encloses all fascicles to form the nerve.
Classification of Nerves
Nerves are classified by the direction of impulse transmission:
Mixed nerves: Contain both sensory (afferent) and motor (efferent) fibers; most common type.
Sensory (afferent) nerves: Carry impulses toward the CNS.
Motor (efferent) nerves: Carry impulses away from the CNS.
Types of fibers in mixed nerves include:
Somatic afferent: Sensory from muscle to brain.
Somatic efferent: Motor from brain to muscle.
Visceral afferent: Sensory from organs to brain.
Visceral efferent: Motor from brain to organs.
Cranial Nerves
Overview of Cranial Nerves
There are 12 pairs of cranial nerves, each with specific sensory, motor, or mixed functions. They are numbered I–XII from rostral to caudal and primarily serve the head and neck (except the vagus nerve, which extends into the thorax and abdomen).
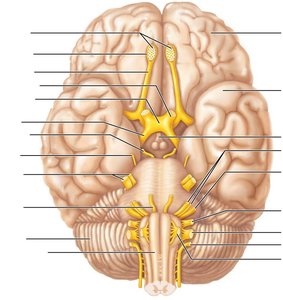
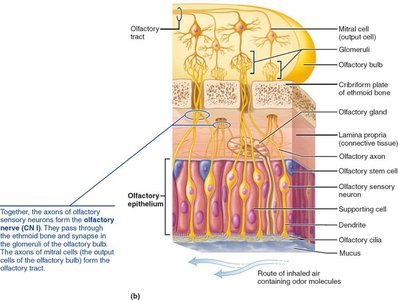
Cranial Nerve I: Olfactory Nerve
The olfactory nerve is responsible for the sense of smell. It runs from the nasal mucosa to the olfactory bulbs, where fibers synapse and then project to the primary olfactory cortex.
Function: Purely sensory (smell).
Clinical relevance: Damage can cause anosmia (loss of smell).
Cranial Nerve II: Optic Nerve
The optic nerve transmits visual information from the retina to the brain. Fibers partially cross at the optic chiasma, continue as optic tracts to the thalamus, and then project to the visual cortex.
Function: Purely sensory (vision).
Clinical relevance: Damage can cause blindness or visual field defects (anopsias).

Cranial Nerves III, IV, VI: Oculomotor, Trochlear, and Abducens Nerves
These nerves control eye movements:
Oculomotor (III): Motor to most extrinsic eye muscles, controls pupil constriction and lens shape (parasympathetic fibers).
Trochlear (IV): Motor to the superior oblique muscle (depresses and rotates the eye).
Abducens (VI): Motor to the lateral rectus muscle (abducts the eye).

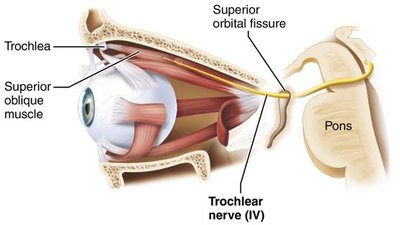
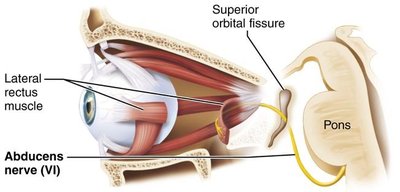
Clinical relevance: Damage to these nerves can result in double vision, inability to move the eye in certain directions, ptosis (drooping eyelid), or strabismus (misalignment of the eyes).
Cranial Nerve V: Trigeminal Nerve
The trigeminal nerve is the largest cranial nerve and has three divisions: ophthalmic (V1), maxillary (V2), and mandibular (V3). It conveys sensory information from the face and supplies motor fibers for mastication (chewing).
Ophthalmic (V1): Sensory from scalp, upper eyelid, nose, cornea.
Maxillary (V2): Sensory from cheek, upper lip, lower eyelid, upper teeth.
Mandibular (V3): Sensory from lower teeth, chin, anterior tongue; motor to chewing muscles.
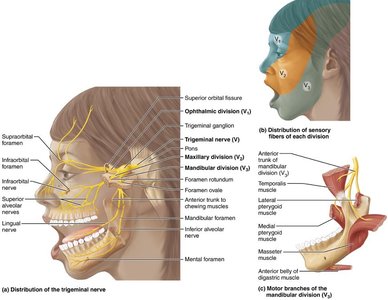
Clinical relevance: Trigeminal neuralgia causes severe facial pain, often triggered by mild stimuli.
Cranial Nerve VII: Facial Nerve
The facial nerve controls muscles of facial expression, conveys taste from the anterior two-thirds of the tongue, and supplies parasympathetic fibers to lacrimal and salivary glands.
Motor: Facial expression, blinking, inner ear reflexes.
Sensory: Taste from anterior tongue.
Parasympathetic: Lacrimal and salivary glands.
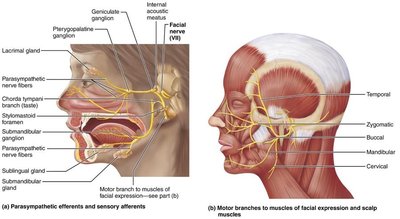
Clinical relevance: Bell's palsy is facial paralysis due to inflammation of the facial nerve.
Cranial Nerve VIII: Vestibulocochlear Nerve
This nerve transmits auditory and equilibrium information from the inner ear to the brain.
Cochlear division: Hearing.
Vestibular division: Balance.
Clinical relevance: Damage can cause deafness, dizziness, loss of balance, and nausea.
Cranial Nerve IX: Glossopharyngeal Nerve
The glossopharyngeal nerve innervates part of the tongue and pharynx, is involved in swallowing, taste, and monitors blood pressure and gas levels via baroreceptors and chemoreceptors.
Clinical relevance: Damage impairs swallowing and taste.
Cranial Nerve X: Vagus Nerve
The vagus nerve is the only cranial nerve to extend beyond the head and neck, innervating thoracic and abdominal organs. It regulates heart rate, breathing, and digestive tract activity.
Clinical relevance: Damage can cause hoarseness, swallowing difficulties, and impaired visceral organ function.
Cranial Nerve XI: Accessory Nerve
The accessory nerve innervates the sternocleidomastoid and trapezius muscles, facilitating head and neck movement.
Clinical relevance: Injury causes weakness in head rotation and shoulder elevation.
Cranial Nerve XII: Hypoglossal Nerve
The hypoglossal nerve controls tongue movements essential for chewing, swallowing, and speech.
Clinical relevance: Damage causes tongue deviation and atrophy, speech and swallowing difficulties.
Spinal Nerves and Dermatomes
Spinal Nerves
There are 31 pairs of spinal nerves, all mixed nerves named for their point of origin from the spinal cord. They supply the body except for the head and part of the neck.
8 pairs cervical (C1–C8)
12 pairs thoracic (T1–T12)
5 pairs lumbar (L1–L5)
5 pairs sacral (S1–S5)
1 pair coccygeal (Co1)
Dermatomes
Dermatomes are regions of skin innervated by sensory fibers of a single spinal nerve. Mapping dermatomes is clinically important for diagnosing nerve or spinal cord injuries.
Organization of the Spinal Cord Gray Matter
The spinal cord gray matter is organized into dorsal (sensory) and ventral (motor) horns, with interneurons and motor neurons arranged by function.
Dorsal horn: Receives sensory input.
Ventral horn: Contains motor neurons.
Dorsal root ganglia: Contain cell bodies of sensory neurons.
Autonomic ganglia: Contain cell bodies of autonomic motor neurons.
Additional info: For more details on the autonomic nervous system, refer to ANS-specific lectures and chapters.
