 Back
BackPhysiology of Blood Flow and Blood Pressure Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Hemodynamics: Physiology of Blood Flow
Introduction to Hemodynamics
Hemodynamics is the study of the forces involved in circulating blood throughout the cardiovascular system. Blood flow is driven by gradients—differences in concentration, pressure, or electrical charge. The heart generates a pressure gradient, with the highest pressure near the heart and decreasing pressure as blood moves through the vasculature. Blood flows from areas of higher pressure to areas of lower pressure.
Blood Pressure: The outward force that blood exerts on the walls of blood vessels, measured in millimeters of mercury (mm Hg). Blood pressure is highest in large systemic arteries and lowest in large systemic veins. (120 mmHg in large systemic arteries, 10-15 mmHg in lower systemic veins).
Blood Flow: The volume of blood that moves per minute, generally matching cardiac output (about 5–6 liters/min in adults). Blood flow is directly proportional to the pressure gradient and inversely proportional to resistance.
Blood flow is directly proportional to the pressure gradient, meaning that blood flow increases when the pressure gradient increases and vice versa.
Blood flow is inversely proportional to resistance; that is, as resistance increases, blood flow decreases.
Resistance: Any impedance to blood flow. As resistance increases, blood flow decreases.
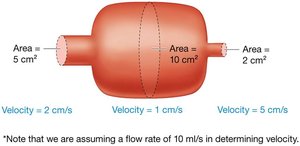
Velocity of Blood Flow: Determined by the cross-sectional area of blood vessels. As vessels branch and total cross-sectional area increases, velocity decreases. This allows efficient exchange of gases and nutrients in capillaries.
The velocity of blood flow is fastest in the aorta and slowest in the capillaries.
Cross-Sectional Area and Velocity
The cross-sectional area of a vessel is calculated as the area of a circle: . Although individual arterioles and capillaries have small radii, their large numbers result in a much greater total cross-sectional area compared to larger vessels.
Example: One large vessel with an area of 5 cm2 versus five smaller vessels each with an area of 2 cm2 (total 10 cm2).
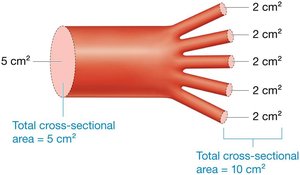
As cross-sectional area increases, blood velocity decreases. This is crucial for capillary exchange.
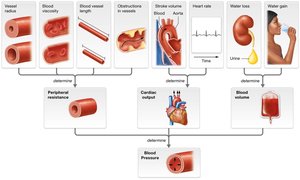
Factors That Determine Blood Pressure
Peripheral Resistance
Peripheral resistance is the opposition to blood flow offered by the blood vessels, primarily in the body's periphery.
Peripheral resistance and blood pressure are directly related: As peripheral resistance increases, blood pressure increases.
Vessel radius is the quickest to change the blood pressure
Vessel length is the slowest to change blood pressure
It is influenced by several factors:
Blood Vessel Radius: Resistance varies inversely with vessel radius. As radius increases (dilation), resistance decreases, and vice versa.

Blood Viscosity: The inherent resistance of a liquid to flow. Blood's high viscosity, due to proteins and cells, increases resistance.
The more viscous a liquid is, the more its molecules resist being put into motion and staying in motion
Blood viscosity remains relatively constant, but it can be altered by states that change either the number of cells or proteins in the blood or the amount of water in the blood, such as dehydration
Peripheral resistance is raised by conditions that increase blood viscosity and is lowered by conditions that decrease blood viscosity.
Blood Vessel Length: Longer vessels present greater resistance. This is one reason why resistance is lower in the pulmonary circuit than in the systemic circuit.
The longer the blood vessel, the greater the resistance.
More pressure is needed to propel blood through a long vessel than a short one

Presence of Obstructions within the Blood Vessels: Caused by certain disease states. Ex. Tumors, the fatty plaques seen with atherosclerosis, or blood clots. This causes Turbulent Blood flow instead of laminar (layered/easy flow)
Turbulent flow = blood doesn’t move forward readily and requires more force to move through the vessels, which increases resistance.
Turbulent blood flow often does as the blood bounces along the vessel walls
These sounds are heard in the heart as murmurs and in the vessels as bruits.
Cardiac Output
Cardiac output (CO) is the product of stroke volume (amount of blood pumped per beat) and heart rate (beats per minute):
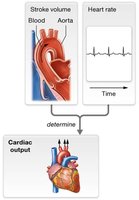
Cardiac output and peripheral resistance are the two factors that determine the pressure gradient driving circulation.
This relationship indicates that anything changing cardiac output is also going to alter the pressure gradient that drives blood flow and therefore the blood pressure.
Increased cardiac output raises blood pressure, while decreased cardiac output lowers it.
Ex. In response to sympathetic nervous system stimulation and the intake of drugs such as caffeine (increase)
Cardiac output decreases in response to parasympathetic nervous system stimulation and drugs that block the sympathetic response. (decrease)
Blood Volume
The total volume of blood in the circulatory system is directly related to the amount of water in the blood. More water increases blood volume and, consequently, blood pressure.
Small increases in blood volume are buffered by the compliance (stretchiness) of veins.
Veins are the most compliant vessels—when blood volume increases, they stretch to accommodate the added fluid, with only a small rise in pressure
When the veins cannot stretch further to accommodate additional increases in blood volume, the extra blood shifts to the arteries.
Arteries are much less compliant, and when blood volume increases in arteries, overall blood pressure rises
Anything that decreases the compliance of arteries or veins, such as normal changes that occur with aging, makes the vasculature less able to adapt to increases in blood volume

Summary Table: Factors Determining Blood Pressure
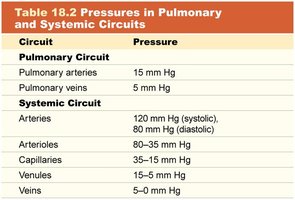
Blood Pressure in Different Portions of the Circulation
Systemic and Pulmonary Circuits
The cardiac outputs of the right and left ventricles are equal under normal conditions, but the resistance in the systemic circuit is far greater than that in the pulmonary circuit
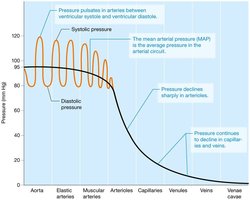
Blood pressure is much lower in the pulmonary circuit (average 15 mm Hg) than in the systemic circuit (average 95 mm Hg). Systemic arterial pressure is highest in the aorta and elastic arteries, declining as blood moves through the system.
Generally, when someone reports his or her “blood pressure,” the person is actually reporting the pressure in the systemic arterial circuit.
Mean Arterial Pressure (MAP): The average pressure in systemic arteries during the cardiac cycle, calculated as:
Because the heart has both contraction and relaxation periods, the pressure gradient generated by the heart pulsates It rises during ventricular systole and declines during ventricular diastole. This leads to two separate pressures in the arteries:
Systolic Pressure: The peak pressure during ventricular contraction (about 120 mm Hg at rest).
Diastolic Pressure: The lowest pressure during ventricular relaxation (about 80 mm Hg at rest).
Pulse Pressure: The difference between systolic and diastolic pressures (about 40 mm Hg).
Pressure in the systemic circuit declines most sharply in the arterioles
MAP decreases from about 80 mm Hg in the large arterioles to about 30 mm Hg in the smallest arterioles
This sharp decrease in pressure is due to the sharp increase in peripheral resistance in the arterioles.
Measuring the Arterial Blood Pressure
When blood flow through the brachial artery resumes at the systolic pressure, it becomes turbulent. This produces audible sounds of Korotkoff that may be auscultated (listened to) with a stethoscope.
The pressure at which the sounds are first auscultated is recorded as the systolic pressure.
Diastolic pressure is often recorded at the point when the sounds disappear.
Calculating the Mean Arterial Pressure
The heart spends more time in diastole than in systole, and this affects the MAP
MAP= Diastolic Pressure + 1/3 (Pulse Pressure)
Ex. Person's BP is 120/80
MAP= 80mmHg + 1/3 (120mmHg-80mmHg)
= 93mmHg
Pressure Changes in the Systemic Circuit
As blood moves from arteries to arterioles, capillaries, venules, and veins, pressure steadily declines. This is due to the branching of vessels and the compliance of veins.
This pressure decrease is largely due to the reduction in blood volume that takes place in capillaries
Pressure declines even further in venules and veins, dropping to only about 4 mm Hg in the inferior vena cava and as low as 0 mm Hg in the right atrium
The low pressure is largely due to the high compliance of veins and the declining resistance as these vessels merge and become larger.
Circuit | Pressure |
|---|---|
Pulmonary arteries | 15 mm Hg |
Pulmonary veins | 5 mm Hg |
Systemic arteries | 120 mm Hg (systolic), 80 mm Hg (diastolic) |
Arterioles | 80–35 mm Hg |
Capillaries | 35–15 mm Hg |
Venules | 15–5 mm Hg |
Veins | 5–0 mm Hg |
Venous Return Mechanisms
Venous blood returns to the heart at the same rate it is pumped into arteries, despite low pressure. Several mechanisms assist venous return:
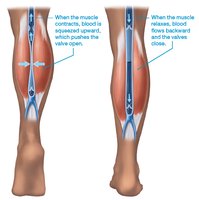
Venous Valves: Prevent backflow of blood in veins.
Smooth Muscle Contraction: Increases venous return under sympathetic stimulation.
Skeletal Muscle Pump: Skeletal muscles surrounding deep veins contract and relax, propelling blood toward the heart.
Respiratory Pump: Changes in thoracic and abdominal pressure during breathing help move blood through veins.
Clinical Application: Varicose Veins and Hemorrhoids
Varicose Veins
Varicose veins are dilated, bulging, and often hardened veins, typically in the superficial veins of the lower limb. They result from conditions that decrease venous return, such as prolonged standing, pregnancy, or abdominal obesity, causing blood to pool and veins to stretch. Superficial veins are more susceptible due to lack of support from skeletal muscle pumps.
Hemorrhoids
Hemorrhoids are varicose veins in the anal region, often caused by increased abdominal pressure during defecation or childbirth. These veins are superficial and not well supported, making them prone to dilation under high pressure.
