 Back
BackPregnancy, Childbirth, and Lactation: ANP Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Pregnancy, Childbirth, and Lactation
Overview
This section covers the physiological and anatomical changes that occur during pregnancy, the process of childbirth, and the mechanisms of lactation. These topics are essential for understanding human development and reproductive physiology in anatomy and physiology courses.
Pregnancy
General Features of Pregnancy
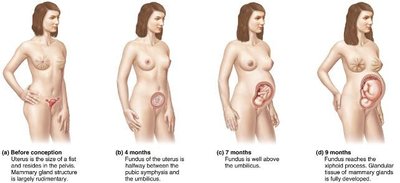
Pregnancy is a complex physiological state that lasts an average of 266 days from conception to childbirth, but is usually measured from the first day of the last menstrual period (LMP), making the typical gestation period about 280 days (40 weeks). Pregnancy is divided into three trimesters, each lasting approximately three months. During this time, nearly every organ system in the mother's body undergoes significant changes to support fetal development.
Metabolism and Nutritional Needs: Increased metabolic rate and nutritional requirements to support fetal growth.
Gastrointestinal System: Changes in motility and absorption, often resulting in symptoms such as nausea and constipation.
Urinary System: Increased urine production and frequency due to higher blood volume and fetal waste disposal.
Respiratory System: Increased tidal volume and possible dyspnea due to diaphragmatic displacement.
Cardiovascular System: Increased blood volume and cardiac output to supply both mother and fetus.
Metabolic and Hormonal Changes
Placental Growth Hormone: Replaces maternal growth hormone, increases lipolysis and gluconeogenesis to provide nutrients for the fetus.
Human Placental Lactogen (hPL): Promotes fetal growth, breast maturation, and exerts glucose-sparing effects in the mother, which can lead to gestational diabetes.
Corticotropin-Releasing Hormone (CRH): Increases toward the end of pregnancy, raising maternal ACTH and cortisol levels for stress protection and fetal lung maturation.
Vitamin D: Levels rise to ensure adequate calcium for fetal bone mineralization.
Physiological Changes by System
Gastrointestinal: Morning sickness, heartburn, and constipation are common due to hormonal and anatomical changes.
Urinary: Increased frequency and urgency due to higher blood volume and fetal pressure on the bladder.
Respiratory: Nasal congestion, increased tidal volume, and dyspnea may occur.
Cardiovascular: Blood volume increases up to 40%, cardiac output rises, and venous return from lower limbs may be impaired, causing edema and varicose veins.
Childbirth (Parturition)
Preparation for Childbirth
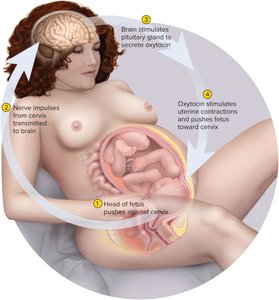
The uterus increases dramatically in size during pregnancy, mainly due to hypertrophy of the myometrium. Contractility increases toward the end of pregnancy, influenced by a rising estrogen-to-progesterone ratio and increased oxytocin secretion from the pituitary gland. Oxytocin is the primary hormone stimulating uterine contractions.
Labor Contractions and Positive Feedback
Initiation: Stretching of the cervix triggers uterine contractions, which push the fetus further into the cervix, amplifying the cycle via a positive feedback loop involving oxytocin.
Hormonal Induction: Fetal CRH and cortisol, placental estrogens, and prostaglandins all contribute to the onset of labor.
Stages of Labor
1. Dilation Stage: Cervical canal widens and thins (effacement), typically to about 10 cm. Amniotic fluid is usually discharged ("water breaking"). Lasts 8–24 hours for first-time mothers.
2. Expulsion Stage: Begins when the baby's head enters the vagina and ends with delivery. Lasts 30–60 minutes for first-time mothers.
3. Placental Stage: Uterus continues to contract, expelling the placenta and fetal membranes (afterbirth).
Postpartum Changes
Physiological Recovery
The first six weeks postpartum are marked by the stabilization and return of the mother's anatomy and physiology to pre-pregnancy conditions. Uterine involution (shrinkage) is achieved through autolysis of uterine cells. Breastfeeding accelerates involution by suppressing estrogen and stimulating oxytocin, which causes uterine contractions.
Lactation
Milk Synthesis and Ejection
Lactation: The synthesis and ejection of milk from the mammary glands, which can last from a week (if not breastfeeding) to several years (if breastfeeding continues).
Stimulation: Mechanically stimulated by nursing or breast pumps.
Average Duration: Most children are breastfed up to age 2.8 years.
Colostrum and Milk Synthesis
Colostrum: Produced in the first 1–3 days postpartum, high in protein and antibodies, but lower in fat than mature milk.
Milk Synthesis: Prolactin is secreted by the pituitary gland starting at 5 weeks of pregnancy, but placental steroids inhibit milk production until after birth. After birth, prolactin stimulates milk synthesis, with levels spiking after each feeding.
Milk Production: Nursing mothers produce about 1.5 L of milk per day and must adjust their diet to meet increased nutritional demands.
Lactation and Ovulation: Lactation suppresses ovulation, providing a natural (though not foolproof) form of contraception.
Milk Type | Timing | Key Features |
|---|---|---|
Colostrum | Days 1–3 postpartum | High in protein and antibodies, low in fat |
Mature Milk | After day 3 | Higher fat content, supports infant growth |
Example: If a mother does not breastfeed, lactation typically ceases within a week. If breastfeeding continues, milk production can persist for years.
Additional info: The positive feedback mechanism of milk ejection involves the hormone oxytocin, which is released in response to suckling and causes contraction of myoepithelial cells in the mammary glands, leading to milk letdown.
