 Back
BackPregnancy, Growth, and Development: Human Anatomy & Physiology Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 23: Pregnancy, Growth, and Development
Overview of Development
Human development begins with fertilization and continues through a series of well-defined stages, culminating in birth and postnatal growth. This chapter explores the processes of fertilization, embryonic and fetal development, and the physiological changes that occur during pregnancy and aging.
Fertilization and Early Development
Fertilization
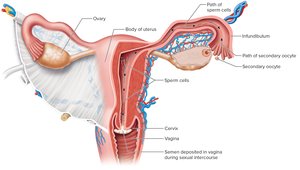
Fertilization is the union of a secondary oocyte and a sperm cell, typically occurring in the infundibulum of the uterine (fallopian) tube. This process initiates the formation of a zygote, marking the beginning of pregnancy.
Transport of Sex Cells: The secondary oocyte must be ovulated and enter the uterine tube, while sperm travel from the vagina through the cervix and uterus to reach the oocyte.
Survival Times: The oocyte survives 12–24 hours after ovulation; sperm can survive up to 6 days in the female reproductive tract.
Fertilization Event: Only one sperm out of millions will penetrate the oocyte's membrane and fertilize it, forming a zygote with 46 chromosomes.
Mechanism of Fertilization
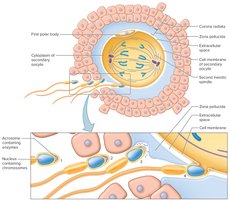
Corona Radiata: The sperm first invade the corona radiata, a layer of follicular cells surrounding the oocyte, using acrosomal enzymes to dissolve it.
Zona Pellucida: Sperm then digest the zona pellucida, a glycoprotein layer closely surrounding the oocyte.
Prevention of Polyspermy: Once a sperm penetrates, the zona pellucida hardens to prevent entry of additional sperm.
Completion of Meiosis II: The secondary oocyte completes meiosis II, forming a polar body and a large cell with the female's chromosomes.
Pronuclei Fusion: The nuclei of the sperm and oocyte (pronuclei) unite, completing fertilization.
Cleavage and Blastocyst Formation
After fertilization, the zygote undergoes rapid mitotic divisions called cleavage, resulting in progressively smaller cells called blastomeres.
Morula: A solid mass of about 16 cells that moves into the uterus.
Blastocyst: A hollow ball of cells that attaches to the endometrium. The inner cell mass gives rise to the embryo proper, while the trophoblast forms structures that support the embryo and secretes human chorionic gonadotropin (hCG).

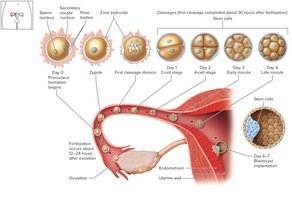
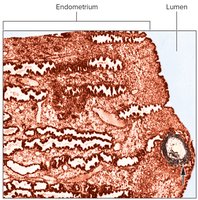
Implantation
Implantation is the attachment of the blastocyst to the uterine lining, occurring between the end of the first and second week after fertilization.
Enzymatic Invasion: The blastocyst secretes proteolytic enzymes to digest part of the endometrium, allowing the trophoblast to invade and establish contact.
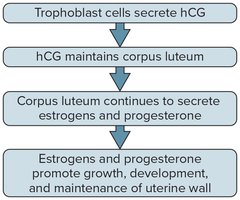
hCG Secretion: The trophoblast produces hCG to maintain the corpus luteum and prevent immune rejection of the blastocyst.
Placenta Formation: The placenta forms from both embryonic and maternal tissues, facilitating nutrient, gas, and waste exchange between mother and embryo.

Assisted Reproductive Technologies (ART)
Intrauterine Insemination: Donated sperm is placed into the cervix or uterus.
In Vitro Fertilization (IVF): Fertilization occurs outside the body, and the embryo is implanted into the uterus.
Gamete Intrafallopian Transfer: Oocytes and sperm are placed together in the uterine tube.
Preimplantation Genetic Diagnosis (PGD)
PGD involves removing one or two cells from a cleavage-stage embryo (after IVF) to test for genetic disorders before implantation.
Application: Used to select embryos free of specific genetic diseases or to obtain stem cells for a sibling with a genetic disorder.

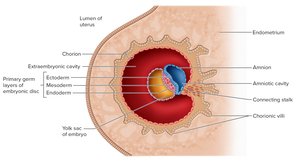
Extraembryonic Membranes and Placentation
Formation of Extraembryonic Membranes
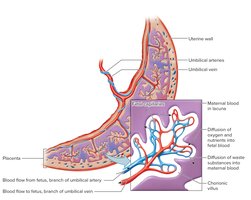
Chorion: Outermost membrane, forms chorionic villi that invade the endometrium and participate in nutrient exchange.
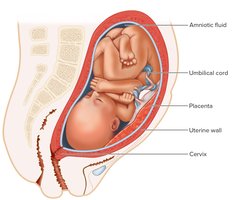
Amnion: Surrounds the embryo, filled with amniotic fluid for protection and temperature regulation.
Yolk Sac: Forms blood cells during early development.
Allantois: Forms blood cells and umbilical blood vessels.
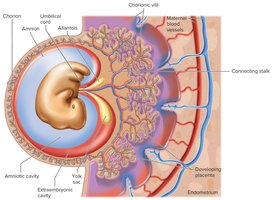
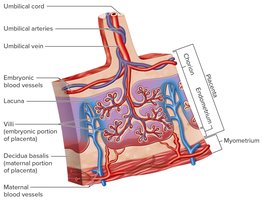
Placenta and Placental Membrane
Placenta: Contains both embryonic (chorion, villi) and maternal (endometrium) portions. It attaches the embryo to the uterine wall and mediates exchange of nutrients, gases, and wastes.
Placental Membrane: Separates maternal and embryonic blood, allowing diffusion but preventing direct mixing.

Embryonic and Fetal Development
Embryonic Stage (Weeks 3–8)
This stage includes gastrulation and organogenesis, during which all major body systems form.
Gastrulation: Formation of three primary germ layers: ectoderm, mesoderm, and endoderm.
Organogenesis: Development of organs from the germ layers.
Critical Period: Most susceptible to teratogens, which can cause congenital malformations.





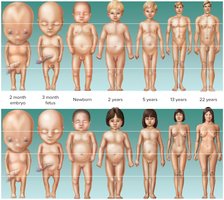
Fetal Stage (Week 9 to Birth)
The fetal stage is characterized by rapid growth and further differentiation of tissues and organs.
Body Proportions: The head is initially large, but the body lengthens and limbs grow.
Organ Maturation: By the end of the fetal stage, all organ systems are functional, though the digestive and respiratory systems mature last.

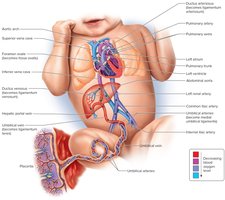
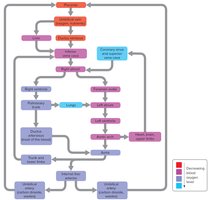
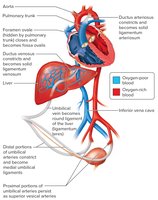
Fetal Circulation
Fetal circulation is adapted to maximize oxygen and nutrient delivery from the mother via the placenta.
Umbilical Vein: Carries oxygen-rich blood from the placenta to the fetus.
Ductus Venosus: Bypasses the fetal liver, connecting the umbilical vein to the inferior vena cava.
Foramen Ovale: Shunts blood from the right atrium to the left atrium, bypassing the nonfunctional fetal lungs.
Ductus Arteriosus: Connects the pulmonary trunk to the aorta, further bypassing the lungs.
Maternal Changes During Pregnancy
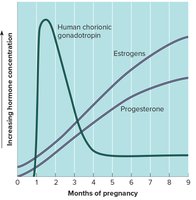
Hormonal Regulation: hCG maintains the corpus luteum, which secretes estrogens and progesterone to support the uterine lining. The placenta eventually takes over hormone production.
Physiological Changes: Increased blood volume, cardiac output, breathing rate, and urine production. The uterus enlarges, displacing abdominal organs.
Nutritional Needs: Increased intake of vitamins, minerals, and proteins is required for both mother and fetus.
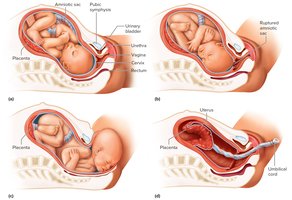
Birth Process (Parturition)
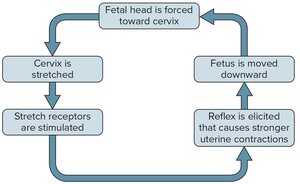
Birth is initiated by hormonal changes, particularly a decrease in progesterone and an increase in prostaglandins, leading to uterine contractions.
Positive Feedback: Stretching of the cervix stimulates oxytocin release, which increases uterine contractions.
Stages of Labor: Dilation of the cervix, expulsion of the fetus, and expulsion of the placenta (afterbirth).
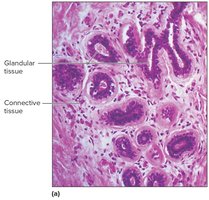
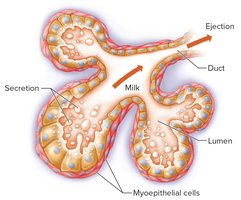
Milk Production and Secretion
Hormonal Control: Estrogens, progesterone, prolactin, and placental lactogen stimulate mammary gland development. Milk secretion begins after birth due to decreased placental hormones.
Colostrum: The first milk, rich in proteins and antibodies, is produced before mature milk.
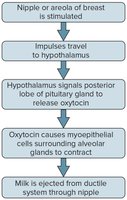
Milk Ejection Reflex: Suckling stimulates oxytocin release, causing milk ejection.
Postnatal Development and Aging
Neonatal Period
The neonatal period (birth to 4 weeks) involves major physiological adjustments, including the initiation of respiration, digestion, and thermoregulation.
Infancy, Childhood, Adolescence, and Adulthood
Infancy: Rapid growth, maturation of systems, and development of motor and communication skills.
Childhood: Continued growth, development of voluntary control, and emotional maturation.
Adolescence: Onset of reproductive capability, secondary sex characteristics, and intellectual/emotional development.
Adulthood: Peak physical function, followed by gradual decline and aging.
Senescence and Aging
Senescence: The process of growing old, involving degenerative changes, reduced cell division, and decreased physiological function.
Passive Aging: Breakdown of structures, loss of elasticity, and accumulation of cellular damage.
Active Aging: Programmed cell death (apoptosis), autoimmunity, and accumulation of metabolic byproducts.
Life Expectancy and End of Life
Life Expectancy: The projected lifespan based on epidemiological data; influenced by genetics, environment, and medical advances.
End of Life: Involves preactive and active dying stages, with progressive loss of physiological function.
