 Back
BackPulmonary Ventilation and Respiratory System Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 16: Pulmonary Ventilation
Overview of Respiration
Respiration is the process by which oxygen is taken into the body and carbon dioxide is expelled. It involves several steps that ensure efficient gas exchange and cellular energy production.
Ventilation: Movement of air between the atmosphere and the lungs.
External Respiration: Exchange of gases between the lungs and the blood.
Internal Respiration: Exchange of gases between the blood and body tissues.
Cellular Respiration: Utilization of oxygen by cells to produce ATP via oxidative phosphorylation.
Respiratory Tract Anatomy
The respiratory tract is divided into the conducting and respiratory zones, each with distinct structures and functions.
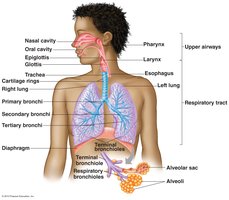
Functions of the Conducting Zone
The conducting zone includes all respiratory passages that serve as airways to the lungs but do not participate in gas exchange.
Air Passageway: Provides a route for air to reach the lungs; volume is about 150 mL (dead space volume).
Air Conditioning: Warms and humidifies incoming air to body temperature and moisture levels.
Particle Removal: Goblet cells secrete mucus to trap particles, while ciliated cells move mucus toward the mouth (mucus escalator).
Function of the Respiratory Zone
The respiratory zone is where gas exchange occurs between air and blood, primarily in the alveoli.
Gas Exchange: Occurs by diffusion across the respiratory membrane.
Respiratory Membrane: Composed of alveolar epithelium, fused basement membrane, and capillary endothelium; only 0.2 microns thick, facilitating rapid diffusion.
Anatomy of Alveoli
Alveoli are the primary sites of gas exchange in the lungs, with specialized cells and structures to optimize this function.
Type I Alveolar Cells: Form the wall of the alveolus; single layer of epithelial cells.
Type II Alveolar Cells: Secrete surfactant to reduce surface tension and prevent alveolar collapse.
Alveolar Macrophages: Engulf and remove debris and pathogens.
Capillary Endothelium: Site of gas exchange with blood; also produces angiotensin-converting enzyme (ACE).

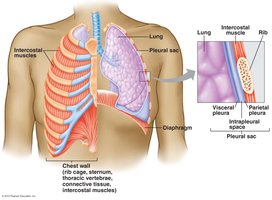
Thoracic Cavity and Pleura
The thoracic cavity houses the lungs and is lined by pleural membranes that facilitate lung movement and reduce friction.
Pleura: Double-layered membrane (visceral and parietal) surrounding each lung.
Pleural Sac: Contains intrapleural fluid, which lubricates and creates surface tension to keep lungs expanded.
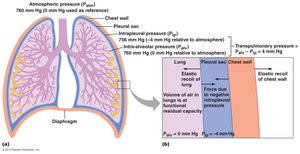
Pulmonary Pressures
Several pressures are involved in pulmonary ventilation, all measured relative to atmospheric pressure (Patm = 0 mm Hg by convention).
Atmospheric Pressure (Patm): Pressure of air outside the body; standard is 760 mm Hg at sea level.
Intra-alveolar Pressure (Palv): Pressure within the alveoli; drives air movement during breathing.
Intrapleural Pressure (Pip): Pressure within the pleural cavity; always negative under normal conditions.
Transpulmonary Pressure: Difference between Palv and Pip; determines lung distension.
Pneumothorax
Pneumothorax occurs when air enters the pleural space, causing lung collapse due to loss of negative intrapleural pressure.

Muscles of Respiration
Breathing involves coordinated action of several muscle groups to change thoracic volume and drive airflow.
Inspiration: Diaphragm and external intercostals contract, increasing thoracic volume.
Expiration: Usually passive; forced expiration involves internal intercostals and abdominal muscles.
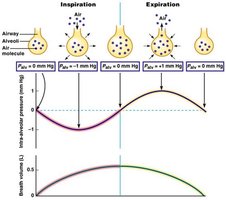
Changes in Intra-Alveolar Pressure During Respiration
Intra-alveolar pressure fluctuates during the respiratory cycle, creating pressure gradients that drive airflow.
Inspiration: Palv drops below Patm, air flows into lungs.
Expiration: Palv rises above Patm, air flows out of lungs.
Lung Compliance and Airway Resistance
Lung compliance and airway resistance are key determinants of the ease of breathing and efficiency of ventilation.
Lung Compliance
Definition: Measure of the lung's ability to stretch and expand.
High Compliance: Easier to inflate lungs; requires less pressure change.
Elasticity: More elastic tissue means less compliance.
Surface Tension: Surfactant from Type II cells reduces surface tension, increasing compliance and making inspiration easier.
Airway Resistance
Definition: Resistance to airflow within the airways; normally low due to large total cross-sectional area.
Increased Resistance: Requires greater pressure gradient for airflow; makes breathing more difficult.
Factors Affecting Airway Resistance
Passive Forces: Transpulmonary pressure and tractive forces during inspiration expand airways.
Mucus Secretion: Increases resistance by narrowing airways.
Smooth Muscle Activity: Bronchoconstriction (narrowing) and bronchodilation (widening) regulated by autonomic nervous system and local factors.
Extrinsic Control: Sympathetic stimulation (epinephrine) causes bronchodilation; parasympathetic causes bronchoconstriction.
Intrinsic Control: Histamine (bronchoconstriction, increased mucus), CO2 (bronchodilation).
Anatomical Dead Space
The conducting zone contains air that does not participate in gas exchange, known as anatomical dead space (about 150 mL).
Lung Volumes and Capacities
Lung volumes and capacities are measured to assess pulmonary function and diagnose respiratory diseases.
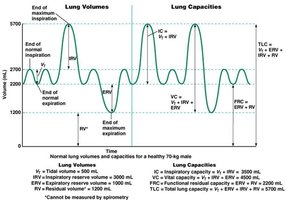
Tidal Volume (VT): Volume of air inhaled or exhaled in a normal breath (~500 mL).
Inspiratory Reserve Volume (IRV): Maximum volume that can be inhaled after a normal inspiration.
Expiratory Reserve Volume (ERV): Maximum volume that can be exhaled after a normal expiration.
Residual Volume (RV): Volume remaining in lungs after maximal exhalation.
Total Lung Capacity (TLC): Sum of all lung volumes.
Vital Capacity (VC): Maximum volume exhaled after maximal inspiration.
Functional Residual Capacity (FRC): Volume in lungs after normal expiration.
Pulmonary Diseases
Obstructive Diseases
Asthma: Spastic contractions of bronchiolar smooth muscle increase airway resistance.
Chronic Obstructive Pulmonary Disease (COPD): Persistent increase in airway resistance; residual volume and total lung capacity increase.
Restrictive Diseases
Definition: Lungs are less able to expand; total lung capacity and vital capacity decrease.
Examples: Polio, tuberculosis.
Pulmonary Function Tests
Forced Vital Capacity (FVC): Maximum volume of air forcibly exhaled after maximal inhalation; low FVC indicates restrictive disease.
FEV1: Percentage of FVC exhaled in 1 second; normal is 80%. FEV1 < 80% suggests obstructive disease.
Minute Ventilation: Total air entering or leaving lungs per minute. Calculated as:
Where is tidal volume and is respiratory rate. For example, .
