 Back
BackRenal Physiology: Filtration, Reabsorption, and Secretion in the Kidney
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Renal System: Physiology and Processes
Overview of Kidney Function
The kidneys are essential organs responsible for filtering blood, removing waste, and maintaining fluid and electrolyte balance. Each day, they process approximately 180 liters of fluid, producing about 1.5 liters of urine. The plasma is filtered around 60 times per day, with less than 1% of the original filtrate excreted as urine. The composition of urine reflects the selective processes of filtration, reabsorption, and secretion.
Filtrate: Plasma minus proteins and cells.
Urine: Contains metabolic wastes and unneeded substances.
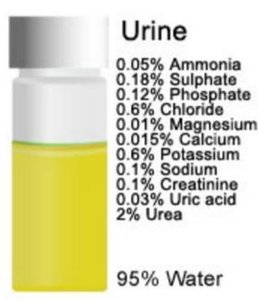
Example: Urine is composed of 95% water, with solutes such as urea, creatinine, sodium, potassium, chloride, and others.
Major Renal Processes
Glomerular Filtration, Tubular Reabsorption, and Tubular Secretion
The nephron, the functional unit of the kidney, carries out three major processes:
Glomerular Filtration: Formation of filtrate from blood.
Tubular Reabsorption: Selective return of substances from filtrate to blood.
Tubular Secretion: Selective transfer of substances from blood to filtrate.
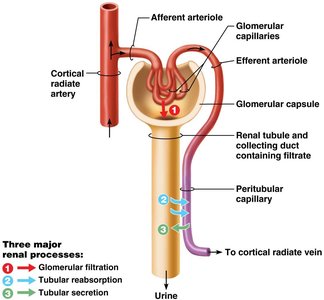
Example: Filtration occurs at the glomerulus, reabsorption and secretion occur along the renal tubule and collecting duct.
Glomerular Filtration
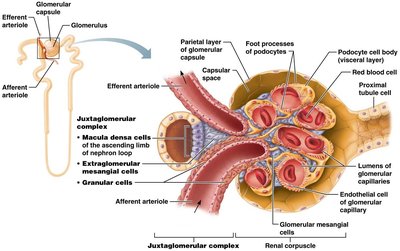
Structure and Function of the Renal Corpuscle
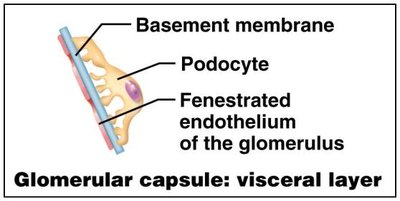
Glomerular filtration is a passive process driven by hydrostatic pressure. The filtration membrane is composed of three layers:
Fenestrated endothelium of glomerular capillaries
Basement membrane
Foot processes of podocytes (visceral layer of glomerular capsule)
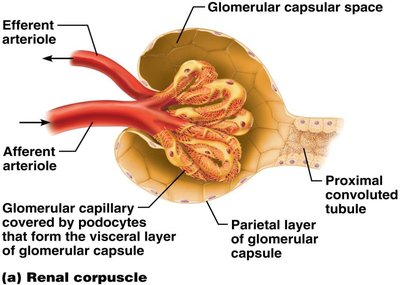
Example: The filtration membrane allows water, glucose, amino acids, and nitrogenous wastes to pass, but retains plasma proteins and cells.
Filtration Membrane Details
The filtration membrane is highly selective, preventing passage of large molecules while allowing small solutes and water.
Filtration slits between podocyte foot processes
Slit diaphragm regulates passage
Fenestrations in capillary endothelium
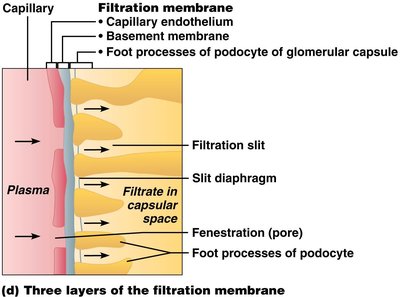
Example: Plasma proteins are retained in the blood, maintaining colloid osmotic pressure.
Pressures Affecting Filtration
Outward and Inward Pressures
Filtration is governed by hydrostatic and osmotic pressures:
Hydrostatic pressure in glomerular capillaries (HPgc): Drives filtrate formation (55 mm Hg).
Hydrostatic pressure in capsular space (HPcs): Opposes filtration (15 mm Hg).
Colloid osmotic pressure in capillaries (OPgc): Opposes filtration (30 mm Hg).
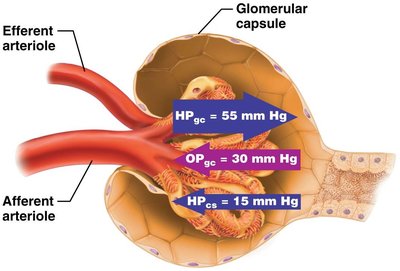
Example: Net filtration pressure (NFP) determines the rate of filtrate formation.
Net Filtration Pressure (NFP)
NFP is calculated as the difference between outward and inward pressures:
Formula:
Example Calculation:
Glomerular Filtration Rate (GFR)
Definition and Clinical Significance
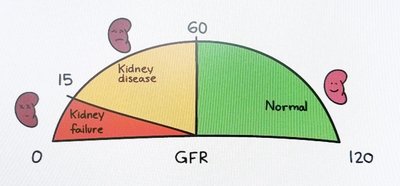
GFR is the volume of filtrate formed per minute by both kidneys. Normal GFR is 120–125 ml/min. GFR is a key indicator of kidney function.
High GFR: May indicate excessive filtration, risk of dehydration.
Low GFR: May indicate kidney disease or failure.
Example: GFR below 60 ml/min suggests kidney disease; below 15 ml/min indicates kidney failure.
Regulation of Glomerular Filtration
Intrinsic Controls: Renal Autoregulation
Intrinsic mechanisms maintain a consistent GFR when mean arterial pressure (MAP) is between 80–180 mm Hg. Two main mechanisms:
Myogenic mechanism: Smooth muscle contracts when stretched, stabilizing GFR.
Tubuloglomerular feedback: Macula densa cells sense Na+ concentration and adjust afferent arteriole diameter.
Example: Increased GFR leads to constriction of afferent arteriole, reducing GFR and allowing more time for Na+ reabsorption.
Extrinsic Controls: Neural and Hormonal Regulation
Extrinsic mechanisms override intrinsic controls to maintain systemic blood pressure, especially during stress or blood loss.
Sympathetic nervous system: Causes vasoconstriction, decreases GFR, increases blood pressure.
Renin-angiotensin-aldosterone system (RAAS): Increases blood pressure by promoting Na+ and water reabsorption.
Example: Renin release is stimulated by sympathetic activity, high Na+ concentration, or reduced stretch in afferent arteriole.
Tubular Reabsorption
Mechanisms and Routes
Tubular reabsorption returns 99% of filtrate to the blood. It occurs via two routes:
Transcellular route: Through tubule cell membranes.
Paracellular route: Between tubule cells, especially in the proximal convoluted tubule (PCT).
Example: Water, Na+, glucose, amino acids, and ions are reabsorbed in the PCT.
Sodium Reabsorption
Sodium is the most abundant cation in filtrate. Its reabsorption is crucial for osmotic balance and occurs via:
Apical membrane: Secondary active transport or facilitated diffusion.
Basolateral membrane: Primary active transport via Na+-K+ ATPase.
Example: Glucose and amino acids are cotransported with Na+.
Water and Solute Reabsorption
Water follows Na+ by osmosis, often through aquaporins. Solute concentration gradients drive passive reabsorption of other substances.
Example: Fat-soluble substances, urea, and some ions are reabsorbed passively.
Nephron Loop and Hormonal Regulation
Concentration of Urine
The nephron loop (loop of Henle) is critical for concentrating urine:
Descending limb: Permeable to water, not solutes.
Ascending limb: Permeable to solutes, not water.
Example: Na+-K+-2Cl– symporters and Na+-H+ antiporters in the thick ascending limb facilitate solute reabsorption.
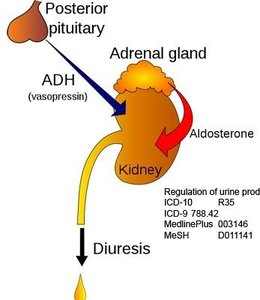
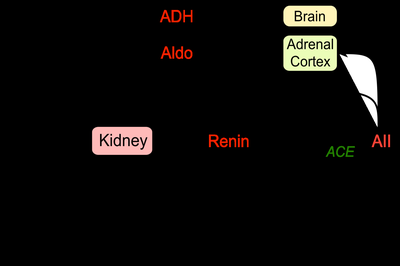
Hormonal Control: ADH and Aldosterone
Antidiuretic hormone (ADH) increases water reabsorption by inserting aquaporins in collecting ducts. Aldosterone increases Na+ reabsorption and decreases K+ levels.
ADH: Less urine, more water retained.
Aldosterone: Essential for life; without it, excessive Na+ loss occurs.
Example: ADH and aldosterone are released in response to dehydration or low blood pressure.
Tubular Secretion
Functions and Importance
Tubular secretion removes substances from blood into filtrate, including drugs, metabolites, excess K+, and H+ ions. It helps regulate blood pH and eliminate waste.
Disposal of bound drugs/metabolites
Elimination of undesirable substances
Regulation of K+ and pH
Example: Aldosterone promotes K+ secretion in exchange for Na+ reabsorption.
Clinical Considerations
Proteinuria and Anuria
Proteinuria indicates a problem with the filtration membrane, allowing proteins to enter filtrate. Anuria is abnormally low urine output, often due to nephron dysfunction.
Proteinuria: Loss of plasma proteins, risk of edema.
Anuria: Less than 50 ml/day urine; may result from acute nephritis or injury.
Example: Kidney stones (renal calculi) are crystallized salts in the renal pelvis.
Summary Table: Urine Composition
Component | Percentage |
|---|---|
Water | 95% |
Urea | 2% |
Chloride | 0.6% |
Potassium | 0.6% |
Sulphate | 0.18% |
Phosphate | 0.12% |
Sodium | 0.1% |
Creatinine | 0.1% |
Ammonia | 0.05% |
Uric acid | 0.03% |
Magnesium | 0.01% |
Calcium | 0.015% |
Example: The composition of urine reflects the selective processes of the nephron.
Additional info: These notes expand upon the original lecture content, providing definitions, examples, and clinical context for renal physiology.
