 Back
BackRespiratory Physiology: Mechanics, Volumes, and Gas Exchange
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System: Physiology
Mechanics of Breathing
The process of pulmonary ventilation involves the movement of air into and out of the lungs, consisting of two phases: inspiration and expiration. These phases are governed by pressure changes within the thoracic cavity.
Inspiration: Gases flow into the lungs as thoracic volume increases.
Expiration: Gases exit the lungs as thoracic volume decreases.
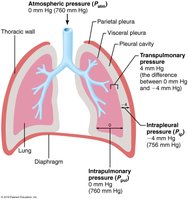
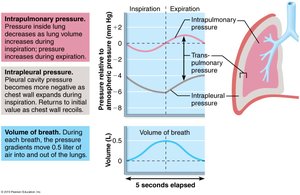
Pressure Relationships in the Thoracic Cavity
Atmospheric Pressure (Patm): The pressure exerted by air surrounding the body, typically 760 mm Hg at sea level.
Intrapulmonary Pressure (Ppul): Pressure within the alveoli, fluctuates with breathing, and eventually equalizes with Patm.
Intrapleural Pressure (Pip): Pressure within the pleural cavity, always negative relative to Patm and Ppul, usually 4 mm Hg less than Ppul. Maintained by the adhesive force between parietal and visceral pleurae.
Transpulmonary Pressure: The difference between Ppul and Pip (), keeps lung spaces open and prevents collapse.
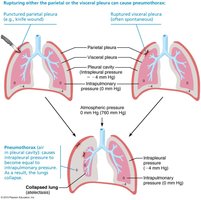
Pneumothorax and Atelectasis
Pneumothorax: Occurs when air enters the pleural cavity, causing Pip to equalize with Patm or Ppul, resulting in lung collapse.
Atelectasis: Collapse of lung tissue due to plugged bronchioles or pneumothorax. Treatment involves removing air with chest tubes.
Pulmonary Ventilation: Volume and Pressure Changes
Pulmonary ventilation is a mechanical process dependent on volume changes in the thoracic cavity, which lead to pressure changes and subsequent airflow.
Boyle’s Law: The relationship between pressure and volume of a gas is inversely proportional: .
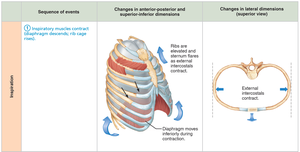
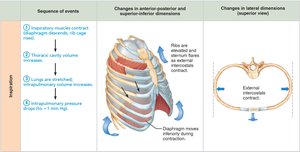
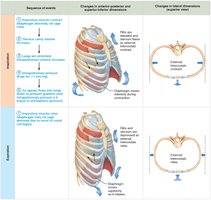
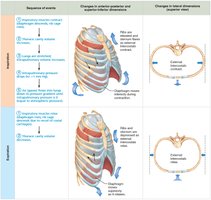
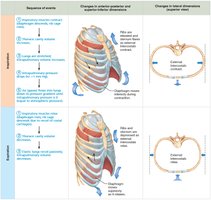
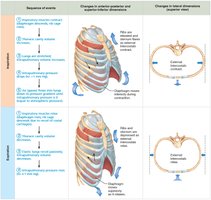
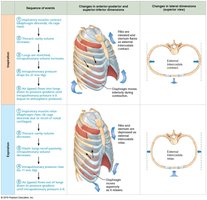
Inspiration
Active Process: Involves contraction of the diaphragm and external intercostals, increasing thoracic volume.
Accessory Muscles: During forced inspiration, muscles such as scalenes, sternocleidomastoid, and pectoralis minor are activated.
Pressure Gradient: As thoracic volume increases, intrapulmonary pressure drops below atmospheric pressure, causing air to flow into the lungs.
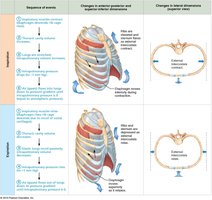


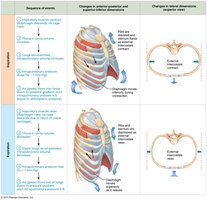
Expiration
Passive Process: Inspiratory muscles relax, thoracic volume decreases, and lungs recoil, increasing intrapulmonary pressure above atmospheric pressure, causing air to flow out.
Forced Expiration: An active process involving abdominal and internal intercostal muscles.
Physical Factors Influencing Pulmonary Ventilation
Three main physical factors affect the ease of air passage and the energy required for ventilation:
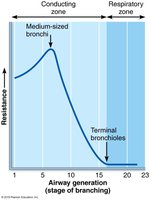
Airway Resistance: Friction in airways is the major nonelastic source of resistance. Resistance is usually insignificant due to large airway diameters and extensive branching. Resistance is highest in medium-sized bronchi and disappears at terminal bronchioles.
Alveolar Surface Tension: The attraction of liquid molecules at the gas-liquid interface tends to collapse alveoli. Surfactant, produced by type II alveolar cells, reduces surface tension and prevents collapse.
Lung Compliance: The measure of lung stretchability, normally high due to distensible tissue and surfactant. Compliance can be diminished by fibrosis, reduced surfactant, or decreased thoracic flexibility.
Assessing Ventilation: Respiratory Volumes and Capacities
Respiratory volumes and capacities are used to assess respiratory status and are measured using spirometry.
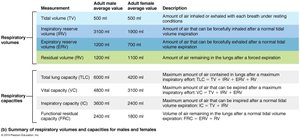
Tidal Volume (TV): Amount of air moved in and out with each breath (~500 ml).
Inspiratory Reserve Volume (IRV): Air inspired forcibly beyond TV (2100–3200 ml).
Expiratory Reserve Volume (ERV): Air expelled forcibly beyond TV (1000–1200 ml).
Residual Volume (RV): Air remaining in lungs after forced expiration, keeps alveoli open.
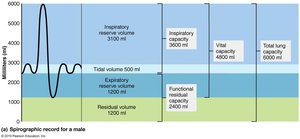
Inspiratory Capacity (IC): TV + IRV
Functional Residual Capacity (FRC): RV + ERV
Vital Capacity (VC): TV + IRV + ERV
Total Lung Capacity (TLC): TV + IRV + ERV + RV
Dead Space
Anatomical Dead Space: Air in passageways not involved in gas exchange (~150 ml).
Alveolar Dead Space: Nonfunctional alveoli due to collapse or obstruction.
Total Dead Space: Sum of anatomical and alveolar dead space.
Pulmonary Function Tests
Obstructive Pulmonary Disease: Increased airway resistance (e.g., bronchitis), TLC, FRC, RV may increase.
Restrictive Disease: Reduced TLC due to disease or environmental exposure (e.g., fibrosis), VC, TLC, FRC, RV decline.
Forced Vital Capacity (FVC): Gas expelled after deep breath.
Forced Expiratory Volume (FEV): Gas expelled during specific interval of FVC.
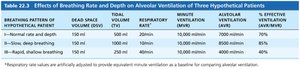
Alveolar Ventilation
Minute Ventilation: Total gas flow in/out of respiratory tract per minute (~6 L/min at rest).
Alveolar Ventilation Rate (AVR): Flow of gases into/out of alveoli per time, calculated as:
Increasing TV is more effective for increasing AVR than increasing frequency.
Gas Exchange: External and Internal Respiration
Gas exchange occurs between lungs and blood (external respiration) and between blood and tissues (internal respiration), governed by partial pressure gradients and gas solubilities.
Basic Properties of Gases
Dalton’s Law: Total pressure of a gas mixture equals the sum of partial pressures of individual gases.
Henry’s Law: Each gas dissolves in liquid in proportion to its partial pressure and solubility.
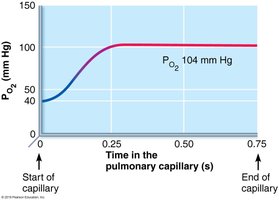
External Respiration
Partial Pressure Gradients: Steep gradient for O2 (drives oxygen into blood), less steep for CO2 (but CO2 is more soluble).
Respiratory Membrane: Thin and large surface area facilitates rapid gas exchange.
Ventilation-Perfusion Coupling: Matching of alveolar ventilation with pulmonary blood perfusion for optimal gas exchange.

Clinical Considerations
Pneumonia/Edema: Increased membrane thickness impairs gas exchange.
Emphysema: Reduced alveolar surface area impairs gas exchange.

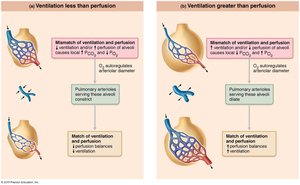
Ventilation-Perfusion Coupling
Perfusion: Blood flow reaching alveoli.
Ventilation: Gas reaching alveoli.
Local PO2 and PCO2 regulate arteriolar and bronchiolar diameters to optimize gas exchange.
Internal Respiration
Partial pressures and diffusion gradients are reversed compared to external respiration.
Oxygen moves from blood to tissues; CO2 moves from tissues to blood.

Summary Table: Respiratory Volumes and Capacities
Measurement | Adult Male Avg. | Adult Female Avg. | Description |
|---|---|---|---|
Tidal Volume (TV) | 500 ml | 500 ml | Air inhaled/exhaled with each breath |
Inspiratory Reserve Volume (IRV) | 3100 ml | 1900 ml | Air forcibly inspired beyond TV |
Expiratory Reserve Volume (ERV) | 1200 ml | 700 ml | Air forcibly expired beyond TV |
Residual Volume (RV) | 1200 ml | 1100 ml | Air remaining after forced expiration |
Total Lung Capacity (TLC) | 6000 ml | 4200 ml | Maximum air in lungs after maximum inspiration |
Vital Capacity (VC) | 4800 ml | 3100 ml | Maximum air expired after maximum inspiration |
Inspiratory Capacity (IC) | 3600 ml | 2400 ml | Maximum air inspired after normal expiration |
Functional Residual Capacity (FRC) | 2400 ml | 1800 ml | Air remaining after normal expiration |
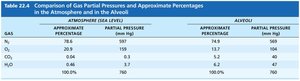
Summary Table: Gas Partial Pressures in Atmosphere and Alveoli
Gas | Atmosphere % | Atmosphere Partial Pressure (mm Hg) | Alveoli % | Alveoli Partial Pressure (mm Hg) |
|---|---|---|---|---|
N2 | 78.6 | 597 | 74.9 | 569 |
O2 | 20.9 | 159 | 14.0 | 104 |
CO2 | 0.04 | 0.3 | 5.2 | 40 |
H2O | 0.5 | 3.7 | 6.2 | 47 |
Total | 100.0 | 760 | 100.0 | 760 |
Summary Table: Effects of Breathing Rate and Depth on Alveolar Ventilation
Breathing Rate | Dead Space Volume (DSV) | Total Volume (TV) | Respiratory Rate | Minute Ventilation | Alveolar Ventilation | % Effective Ventilation |
|---|---|---|---|---|---|---|
Normal rate and depth | 150 ml | 500 ml | 12/min | 6000 ml/min | 4200 ml/min | 70% |
Slow, deep breathing | 150 ml | 1000 ml | 6/min | 6000 ml/min | 5100 ml/min | 85% |
Rapid, shallow breathing | 150 ml | 250 ml | 24/min | 6000 ml/min | 2400 ml/min | 40% |
Key Equations
Boyle’s Law:
Transpulmonary Pressure:
Alveolar Ventilation Rate:
Lung Compliance:
Clinical Applications
Asthma: Increased airway resistance, treated with epinephrine.
Infant Respiratory Distress Syndrome (IRDS): Insufficient surfactant in premature infants, treated with surfactant therapy.
Fibrosis: Nonelastic scar tissue reduces lung compliance.
Emphysema: Reduced alveolar surface area impairs gas exchange.
Additional info: These notes provide a comprehensive overview of respiratory physiology, including mechanics of breathing, physical factors influencing ventilation, assessment of respiratory volumes and capacities, and the principles of gas exchange. Clinical correlations are included to highlight the relevance of these concepts in health and disease.
