 Back
BackRespiratory Physiology: Mechanisms of Pulmonary Ventilation, Gas Exchange, and Transport
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Respiratory Physiology
Overview of Respiration
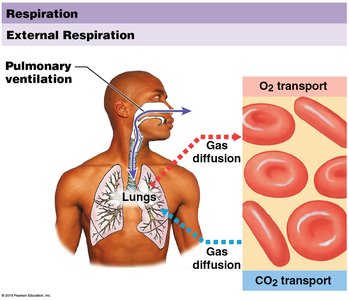
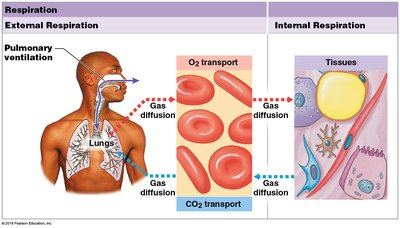
Respiration is a vital process that ensures the exchange of gases (oxygen and carbon dioxide) between the atmosphere, blood, and body tissues. It consists of two integrated processes: external respiration and internal respiration.
External respiration: The exchange of gases between the lungs and the blood.
Internal respiration: The exchange of gases between the blood and the tissues.
External and Internal Respiration
Definitions and Processes
External respiration involves the movement of oxygen from the alveoli into the blood and the removal of carbon dioxide from the blood into the alveoli. This process depends on the partial pressure gradients of O2 and CO2 across the respiratory membrane.
Pulmonary ventilation: The physical movement of air into and out of the lungs, maintaining alveolar ventilation.
Gas diffusion: The movement of O2 and CO2 across the alveolar-capillary membrane.
Internal respiration refers to the exchange of gases between systemic capillaries and tissue cells. Oxygen diffuses from the blood into the tissues, while carbon dioxide moves from the tissues into the blood.
Oxygen absorption: Oxygen is absorbed from the blood by tissue cells.
Carbon dioxide release: Carbon dioxide is released by tissue cells into the blood.
Clinical Relevance: Hypoxia and Anoxia
Hypoxia: Low tissue oxygen levels, which severely limit metabolic activities.
Anoxia: Complete lack of oxygen supply, often resulting in tissue damage, such as that seen in heart attacks and strokes.
Pulmonary Ventilation
Mechanics of Breathing
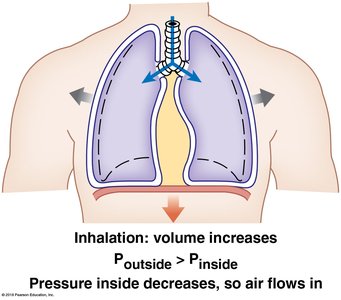
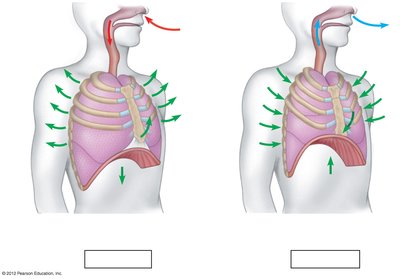
Pulmonary ventilation is driven by changes in thoracic cavity volume, which alter the pressure within the lungs. Air flows from regions of higher pressure to lower pressure.
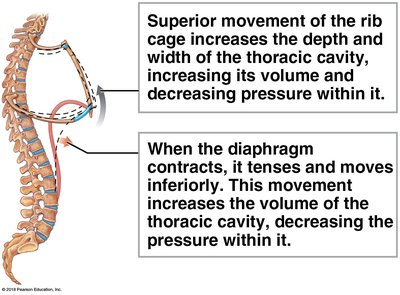
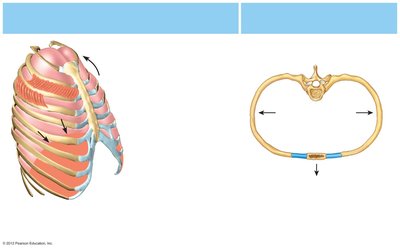
Inhalation (Inspiration): The diaphragm and external intercostal muscles contract, increasing thoracic cavity volume and decreasing intrapulmonary pressure, causing air to flow into the lungs.
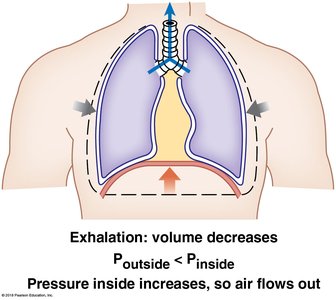
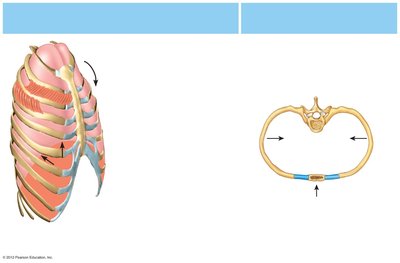
Exhalation (Expiration): The diaphragm and external intercostal muscles relax, decreasing thoracic cavity volume and increasing intrapulmonary pressure, causing air to flow out of the lungs.
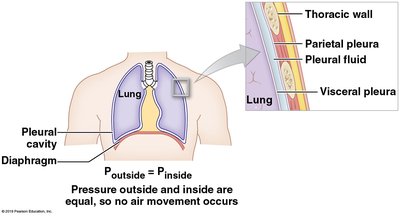
Role of the Pleura
The parietal pleura lines the thoracic wall, while the visceral pleura covers the lungs. Pleural fluid between these layers creates surface tension, allowing the lungs to expand and contract with the thoracic cavity. If air enters the pleural cavity (pneumothorax), the lung may collapse due to loss of this bond.
Muscles of Respiration
Diaphragm: Primary muscle of inspiration; contraction increases thoracic volume.
External intercostals: Elevate the ribs during inspiration.
Internal intercostals and abdominal muscles: Active during forced expiration.
Pulmonary Function Tests
Respiratory Volumes and Capacities
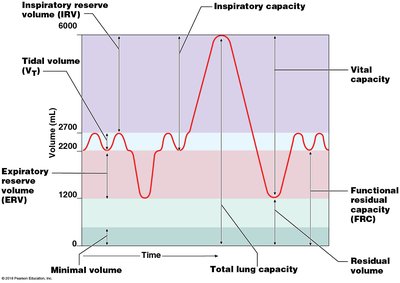
Pulmonary function tests measure the volume and flow of air during breathing. Key volumes and capacities include:
Tidal Volume (VT): Amount of air moved in or out during normal breathing (~500 mL).
Inspiratory Reserve Volume (IRV): Additional air inhaled after a normal inspiration.
Expiratory Reserve Volume (ERV): Additional air exhaled after a normal expiration.
Residual Volume: Air remaining in lungs after maximal exhalation.
Capacities are combinations of volumes:
Inspiratory Capacity:
Vital Capacity:
Functional Residual Capacity (FRC):
Total Lung Capacity:
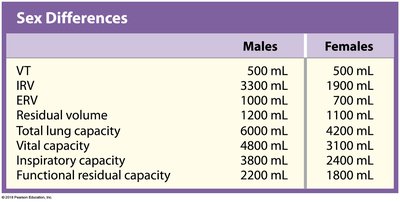
Sex Differences in Respiratory Volumes
Volume/Capacity | Males | Females |
|---|---|---|
VT (Tidal Volume) | 500 mL | 500 mL |
IRV (Inspiratory Reserve Volume) | 3300 mL | 1900 mL |
ERV (Expiratory Reserve Volume) | 1000 mL | 700 mL |
Residual Volume | 1200 mL | 1100 mL |
Total Lung Capacity | 6000 mL | 4200 mL |
Vital Capacity | 4800 mL | 3100 mL |
Inspiratory Capacity | 3800 mL | 2400 mL |
Functional Residual Capacity | 2200 mL | 1800 mL |
Gas Diffusion and Exchange
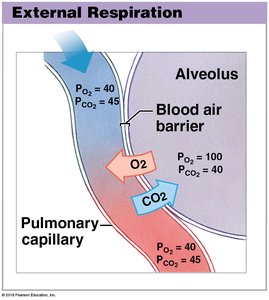
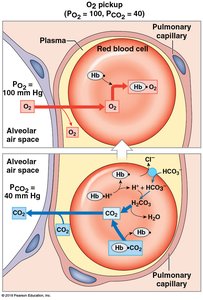
External Respiration (Alveolar Gas Exchange)
Oxygen diffuses from alveoli (high PO2) into pulmonary capillaries (low PO2), while carbon dioxide diffuses from capillaries (high PCO2) into alveoli (low PCO2).
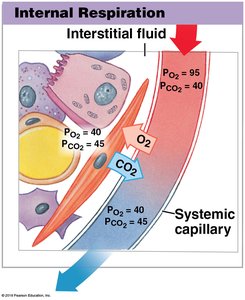
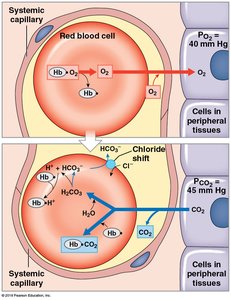
Internal Respiration (Tissue Gas Exchange)
Oxygen diffuses from systemic capillaries (high PO2) into tissues (low PO2), and carbon dioxide diffuses from tissues (high PCO2) into capillaries (low PCO2).
Oxygen and Carbon Dioxide Transport
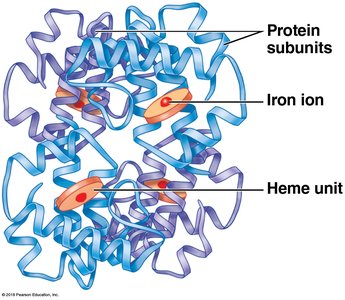
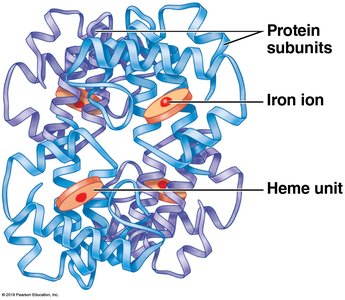
Oxygen Transport
Most oxygen in the blood is transported bound to hemoglobin within red blood cells. Each hemoglobin molecule can bind up to four oxygen molecules, forming oxyhemoglobin (HbO2).
~1.5% of O2 is dissolved in plasma.
~98.5% is bound to hemoglobin.
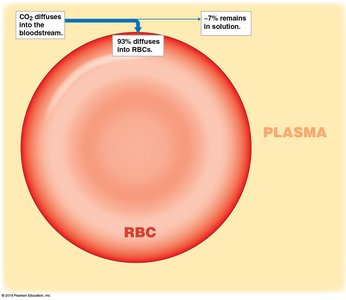
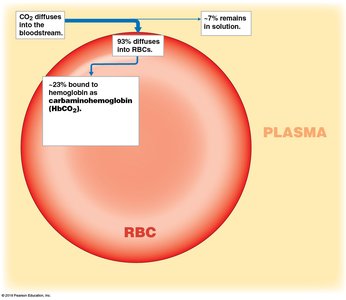
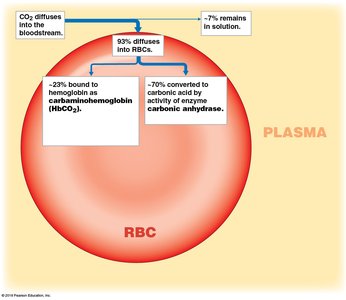
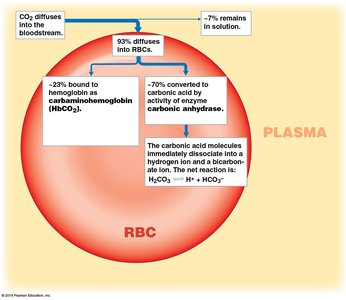
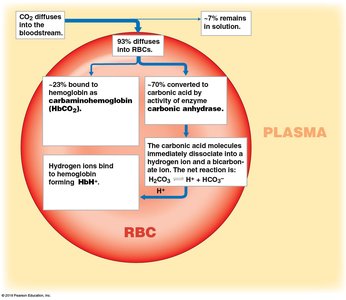
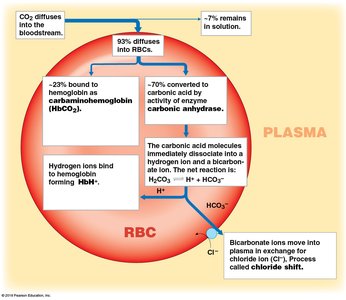
Carbon Dioxide Transport
Carbon dioxide is transported in the blood in three main forms:
Dissolved in plasma (~7%).
Bound to hemoglobin as carbaminohemoglobin (HbCO2) (~23%).
Converted to bicarbonate ion (HCO3−) (~70%) by the enzyme carbonic anhydrase in red blood cells.
Gas Exchange at the Alveoli and Tissues
Gas exchange at the alveoli (external respiration) and at peripheral tissues (internal respiration) involves the coordinated movement of O2 and CO2 between blood, alveoli, and tissues, facilitated by hemoglobin and plasma transport mechanisms.
Neural Regulation of Respiration
Control Centers
The activity of respiratory muscles is regulated by neural centers in the brainstem:
Medulla oblongata: Sets the basic rhythm of breathing and contains the inspiratory center.
Pons: Modifies and smooths out the respiratory rate.
Respiratory rate is normally 12–15 breaths per minute (eupnea). Increased rate (hyperpnea) occurs during increased oxygen demand.
Chemical Regulation
CO2 levels: The primary driver of respiratory rate; increased CO2 (and decreased pH) stimulates increased rate and depth of breathing via chemoreceptors and the medulla.
O2 levels: Detected by chemoreceptors in the aorta and carotid arteries; significant during hypoxia or increased demand.
Hyperventilation (rapid, deep breathing) reduces CO2 and corrects acidosis, while hypoventilation (slow, shallow breathing) allows CO2 to accumulate, correcting alkalosis.
Summary Table: Forms of Gas Transport in Blood
Gas | Transport Form | Percentage |
|---|---|---|
Oxygen (O2) | Bound to hemoglobin | ~98.5% |
Oxygen (O2) | Dissolved in plasma | ~1.5% |
Carbon dioxide (CO2) | Dissolved in plasma | ~7% |
Carbon dioxide (CO2) | Bound to hemoglobin (HbCO2) | ~23% |
Carbon dioxide (CO2) | As bicarbonate ion (HCO3−) | ~70% |
Additional info: The chloride shift is an important mechanism for maintaining ionic balance during CO2 transport. Pulmonary function tests are essential for diagnosing and monitoring respiratory diseases.
