 Back
BackRespiratory System Disorders: Structure, Function, and Pathology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Respiratory System Anatomy and Physiology
Overview of Respiratory Structures
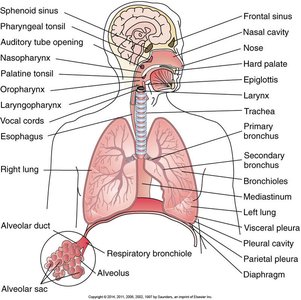
The respiratory system is responsible for gas exchange, supplying oxygen to the blood and removing carbon dioxide. It consists of upper and lower respiratory tracts, including the nasal cavity, pharynx, larynx, trachea, bronchi, bronchioles, and alveoli.
Upper respiratory tract: Nasal cavity, pharynx, larynx
Lower respiratory tract: Trachea, bronchi, bronchioles, alveoli
Alveoli: Primary site of gas exchange
Pleura: Double-layered membrane surrounding the lungs
Mechanics of Ventilation
Ventilation is the process of moving air into and out of the lungs, driven by pressure changes created by the diaphragm and intercostal muscles.
Inspiration: Diaphragm contracts, thoracic cavity expands, intrapulmonary pressure drops, air flows in.
Expiration: Diaphragm relaxes, thoracic cavity volume decreases, intrapulmonary pressure rises, air flows out.
Atmospheric pressure: The pressure exerted by the air surrounding the body, typically 760 mm Hg at sea level.

Pulmonary Volumes
Pulmonary volumes are measurements of air movement during different phases of the respiratory cycle. These values are important for assessing lung function.
Name | Volume | Meaning |
|---|---|---|
Tidal volume (TV) | 500 mL | Amount of air entering lungs with each normal breath |
Residual volume (RV) | 1200 mL | Amount of air remaining in the lungs after forced expiration |
Inspiratory reserve (IRV) | 3000 mL | Maximal amount of air that can be inhaled in excess of normal quiet inspiration |
Expiratory reserve (ERV) | 1100 mL | Maximal volume of air expired following a passive expiration |
Vital capacity (VC) | 4600 mL | Maximal amount of air expired following a maximal inspiration |
Total lung capacity (TLC) | 5800 mL | Total volume of air in the lungs after maximal inspiration |

Pulmonary Capillaries and Alveoli
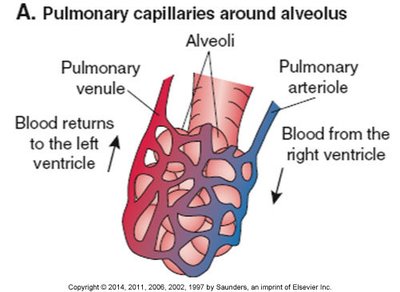
Gas exchange occurs in the alveoli, which are surrounded by a dense network of pulmonary capillaries. Oxygen diffuses from alveoli into blood, while carbon dioxide diffuses from blood into alveoli.
Pulmonary arteriole: Brings deoxygenated blood from the right ventricle to the alveolus.
Pulmonary venule: Returns oxygenated blood to the left ventricle.
Alveolar Structure
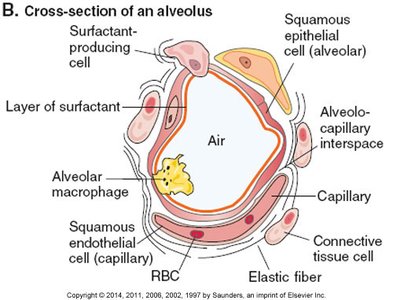
Alveoli are lined with squamous epithelial cells and contain surfactant-producing cells to reduce surface tension, preventing collapse. Alveolar macrophages provide immune defense.
Surfactant: Lipoprotein that reduces surface tension in alveoli.
Alveolar-capillary membrane: Thin barrier for efficient gas exchange.
Diffusion of Gases
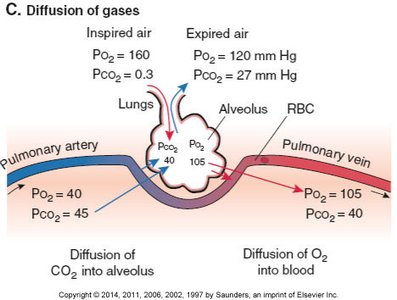
Gas exchange is driven by differences in partial pressures of oxygen (O2) and carbon dioxide (CO2) between alveolar air and blood.
Oxygen: Diffuses from alveoli (high PO2) to blood (low PO2).
Carbon dioxide: Diffuses from blood (high PCO2) to alveoli (low PCO2).
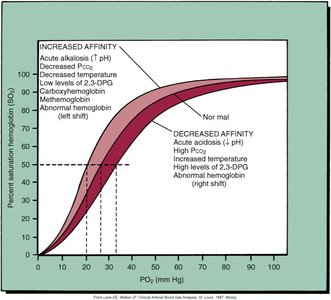
Oxyhemoglobin Dissociation Curve
The oxyhemoglobin dissociation curve describes the relationship between the partial pressure of oxygen (PO2) and hemoglobin saturation. Factors such as pH, temperature, and CO2 levels shift the curve, affecting oxygen release to tissues.
Left shift: Increased affinity (alkalosis, low temperature, low CO2).
Right shift: Decreased affinity (acidosis, high temperature, high CO2).
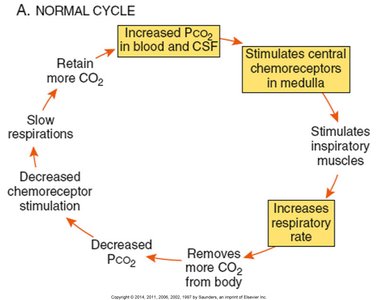
Control of Respiration
Respiratory control centers in the medulla and pons regulate the rate and depth of breathing in response to CO2, O2, and pH levels in the blood.
Central chemoreceptors: Respond to increased CO2 (hypercapnia) and decreased pH.
Peripheral chemoreceptors: Respond to low O2 (hypoxemia).
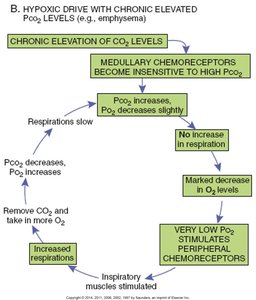
Hypoxic Drive
In chronic respiratory disorders (e.g., emphysema), the body may rely on low O2 levels (hypoxic drive) rather than high CO2 to stimulate breathing.
Chronic CO2 retention: Central chemoreceptors become less sensitive.
Peripheral chemoreceptors: Stimulated by low O2, increasing respiratory rate.
Respiratory Patterns and Diagnostic Tests
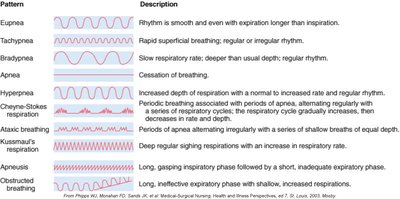
Respiratory Patterns
Various breathing patterns can indicate underlying respiratory pathology.
Pattern | Description |
|---|---|
Eupnea | Normal, smooth, even rhythm |
Tachypnea | Rapid, superficial breathing |
Bradypnea | Slow, deeper than usual breathing |
Apnea | Cessation of breathing |
Hyperpnea | Increased depth of respiration |
Kussmaul's respiration | Deep, rapid breathing (acidosis) |
Cheyne-Stokes respiration | Alternating periods of apnea and deep, rapid breathing |
Obstructed breathing | Long, gasping inspiratory phase, short expiratory phase |
Diagnostic Tests
Several tests are used to diagnose and monitor respiratory diseases:
Spirometry: Measures pulmonary volumes and airflow times.
Arterial blood gas (ABG): Assesses O2, CO2, bicarbonate, and pH.
Oximetry: Measures O2 saturation.
Radiography: Detects tumors, infections, and other abnormalities.
Bronchoscopy: Visualizes airways, allows biopsy.
Culture and sensitivity: Identifies pathogens in sputum.
Therapies for Respiratory Disorders
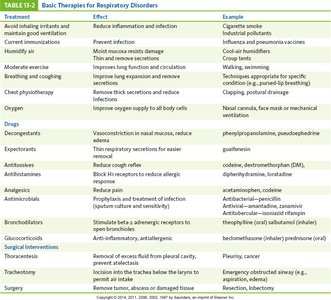
Basic Therapies
Treatment strategies for respiratory disorders include both general and specific interventions.
Treatment | Effect | Example |
|---|---|---|
Avoid irritants | Reduce inflammation and infection | Cigarette smoke |
Immunizations | Prevent infection | Influenza, pneumonia vaccines |
Humidified air | Moistens mucosa, reduces damage | Humidifier |
Chest physiotherapy | Removes thick secretions | Chest percussion |
Oxygen therapy | Improves oxygen supply | Nasal cannula, mask |
Bronchodilators | Dilate bronchioles | Albuterol |
Glucocorticoids | Reduce inflammation | Prednisone |
Antibiotics | Treat infections | Amoxicillin |
Infectious Diseases of the Respiratory System
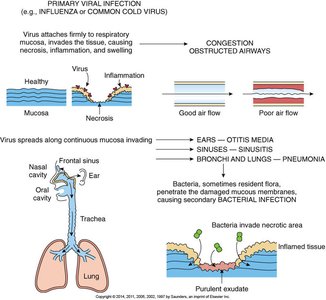
Pathogenesis of Viral Respiratory Infections
Viral infections such as the common cold and influenza can damage respiratory mucosa, leading to secondary bacterial infections.
Primary infection: Virus invades mucosa, causing necrosis and inflammation.
Secondary infection: Bacteria invade damaged tissue, producing purulent exudate.
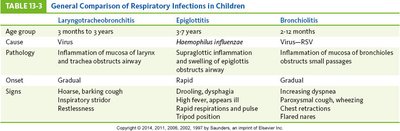
Comparison of Respiratory Infections in Children
Respiratory infections in children vary by age group, causative agent, and clinical presentation.
Laryngotracheobronchitis | Epiglottitis | Bronchiolitis | |
|---|---|---|---|
Age group | 3 months to 3 years | 3-7 years | 2-12 months |
Cause | Virus | Haemophilus influenzae | RSV |
Pathology | Inflammation of mucosa of larynx and trachea | Supraglottic inflammation and swelling | Inflammation of bronchioles |
Onset | Gradual | Rapid | Gradual |
Signs | Barking cough, inspiratory stridor | Drooling, dysphagia, tripod position | Wheezing, chest retractions |
Scarlet Fever
Scarlet fever is caused by group A β-hemolytic Streptococcus (S. pyogenes) and is characterized by a 'strawberry' tongue, fever, and sore throat.
Symptoms: Strawberry tongue, fever, chills, vomiting, abdominal pain, malaise
Treatment: Antibiotics

Pneumonia and Tuberculosis
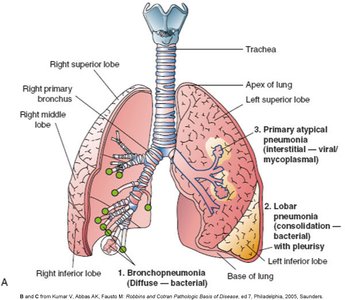
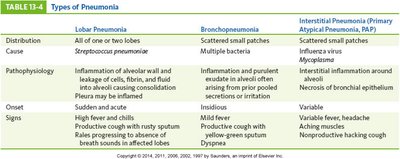
Types of Pneumonia
Pneumonia is classified by causative agent, anatomical location, and pathophysiology.
Lobar pneumonia: Involves one or more lobes, usually caused by Streptococcus pneumoniae.
Bronchopneumonia: Scattered patches, multiple bacteria.
Interstitial (atypical) pneumonia: Scattered small patches, often viral or mycoplasma.
Lobar Pneumonia | Bronchopneumonia | Interstitial Pneumonia | |
|---|---|---|---|
Distribution | All or one/two lobes | Scattered small patches | Scattered small patches |
Cause | Streptococcus pneumoniae | Multiple bacteria | Virus, Mycoplasma |
Onset | Sudden, acute | Insidious | Variable |
Signs | High fever, chills, productive cough | Mild fever, productive cough | Variable fever, headache, nonproductive cough |
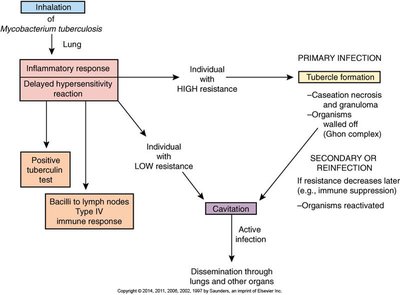
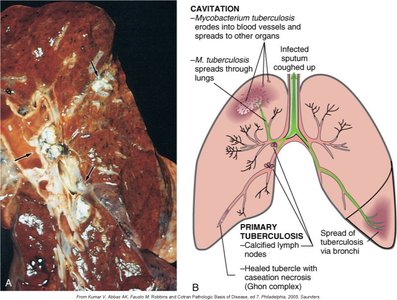
Tuberculosis Pathogenesis
Tuberculosis is caused by Mycobacterium tuberculosis and can result in primary infection (tubercle formation) or secondary/reactivation disease (cavitation and dissemination).
Primary infection: Formation of granulomas (tubercles) in the lung.
Secondary infection: Reactivation leads to cavitation and spread.
Obstructive Lung Diseases
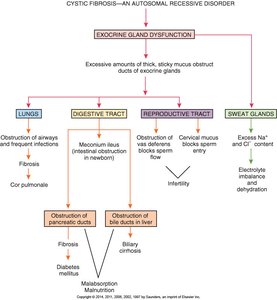
Cystic Fibrosis
Cystic fibrosis is an autosomal recessive disorder causing thick, sticky mucus in the lungs, pancreas, and other organs, leading to chronic infections and malabsorption.
Respiratory: Mucus obstructs bronchioles, frequent infections, chronic cough.
Digestive: Pancreatic duct obstruction, malabsorption, steatorrhea.
Reproductive: Infertility due to mucus obstruction.
Diagnosis: Genetic testing, sweat test, pulmonary function tests.
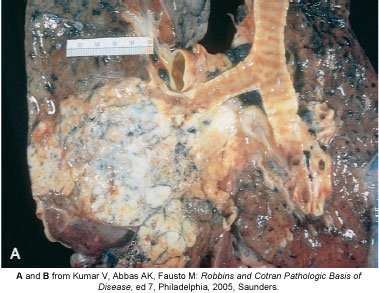
Lung Cancer
Lung cancer, most commonly bronchogenic carcinoma, is strongly associated with smoking. Tumors can obstruct airways, cause hemoptysis, and metastasize.
Types: Squamous cell carcinoma, adenocarcinoma, small cell carcinoma.
Symptoms: Persistent cough, chest pain, weight loss, hemoptysis.
Diagnosis: Imaging, bronchoscopy, biopsy.
Treatment: Surgery, chemotherapy, radiation.
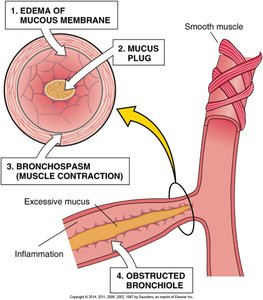
Asthma Pathophysiology
Asthma is a chronic inflammatory disease characterized by bronchial hyperresponsiveness, airway inflammation, and reversible airflow obstruction.
Triggers: Allergens, infections, exercise, cold air, irritants.
Pathology: Mucosal edema, bronchospasm, mucus plugging.
Additional info: This guide covers the structure, function, and common disorders of the respiratory system, integrating clinical and diagnostic perspectives essential for ANP college-level study.
