 Back
BackSkeletal Muscle Tissue: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Skeletal Muscle Tissue
Types of Muscle Tissue
Muscle tissue is classified into three main types, each with distinct structural and functional characteristics:
Cardiac Muscle: Found only in the heart, responsible for propelling blood through blood vessels. It is involuntary and striated.
Smooth Muscle: Located in walls of hollow organs (e.g., digestive tract, arteries). It is involuntary, non-striated, and regulates movement of fluids and solids, as well as vessel diameter.
Skeletal Muscle: Attached to bones, responsible for voluntary movements by pulling on bones. Each cell is a single muscle fiber, and each muscle is an organ containing all four tissue types.

Functions of Skeletal Muscle
Skeletal muscle performs several essential functions in the body:
Produce skeletal movements: Enables locomotion and manipulation of the environment.
Maintain posture and body position: Stabilizes joints and maintains body alignment.
Support soft tissues: Protects internal organs.
Guard entrances and exits: Controls openings of digestive and urinary tracts.
Maintain body temperature: Generates heat during contraction.
Provide nutrient reserves: Stores glycogen and proteins for energy.
Skeletal Muscle Structure
Connective Tissue Components
Three layers of connective tissue organize and protect skeletal muscle:
Epimysium: Dense collagen layer surrounding the entire muscle, connected to deep fascia.
Perimysium: Fibrous layer dividing muscle into fascicles (bundles of cells), containing blood vessels and nerves.
Endomysium: Surrounds individual muscle fibers, contains capillaries, myosatellite cells, and neuron axons.
Tendons and Aponeuroses
Tendons are bundles of collagen fibers that attach muscle to bone, while aponeuroses are sheet-like extensions. All three connective tissue layers merge to form these structures.
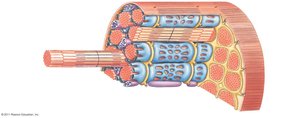
Muscle Fiber Anatomy
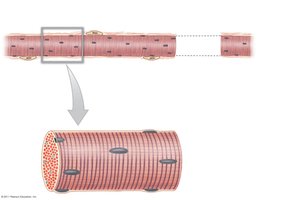
Skeletal muscle fibers are large, multinucleated cells with specialized structures:
Sarcolemma: Plasma membrane of the muscle fiber.
Sarcoplasm: Cytoplasm containing abundant mitochondria for energy production.
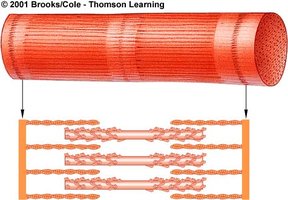
Myofibrils: Cylindrical structures composed of myofilaments (actin and myosin).
Development of Skeletal Muscle
Muscle fibers develop from the fusion of myoblasts, forming multinucleated cells. Some myoblasts remain as myosatellite cells, aiding in muscle repair.

Skeletal Muscle Fiber Structure
Myofibrils and Myofilaments
Myofibrils are composed of repeating units called sarcomeres, which are the functional units of contraction. Each sarcomere contains:
Thin filaments: Primarily actin, attached to Z lines.
Thick filaments: Primarily myosin, anchored at the M line.

Sarcomere Structure
The sarcomere is defined by Z lines and contains several regions:
A band: Dense region with thick filaments.
I band: Region with only thin filaments.
M line: Center of the sarcomere, connecting thick filaments.
H band: Area around the M line with only thick filaments.

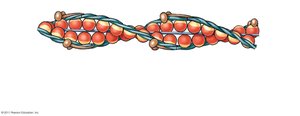
Thin and Thick Filaments
Thin filaments are composed of F-actin (filamentous actin), formed by linking G-actin (globular actin) molecules. Nebulin stabilizes the F-actin strand. Thick filaments are made of myosin, each with a tail and two heads, and contain titin for elasticity.

Regulatory Proteins: Troponin and Tropomyosin
Troponin and tropomyosin regulate muscle contraction:
Tropomyosin: Covers actin active sites, preventing myosin binding.
Troponin: Binds calcium, tropomyosin, and actin; changes shape when calcium binds, moving tropomyosin and exposing active sites.
Muscle Contraction Mechanism
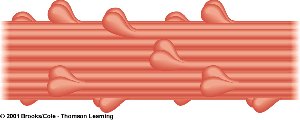
Sliding Filament Theory
Muscle contraction occurs when thin filaments slide past thick filaments, shortening the sarcomere. Myosin heads form cross-bridges with actin, pivot, and pull actin toward the center.

Contraction Cycle Steps
Active-site exposure: Calcium binds to troponin, moving tropomyosin.
Cross-bridge formation: Myosin heads bind to actin.
Power stroke: Myosin head pivots, pulling actin.
Cross-bridge detachment: ATP binds to myosin, releasing it from actin.
Myosin reactivation: ATP is hydrolyzed, re-cocking the myosin head.

Excitation-Contraction Coupling
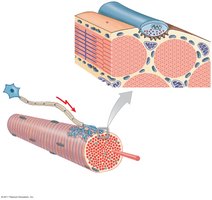
Role of Sarcolemma and T Tubules
The sarcolemma maintains a transmembrane potential. Action potentials travel along T tubules, triggering calcium release from the sarcoplasmic reticulum (SR).
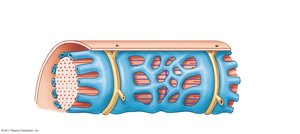
Sarcoplasmic Reticulum (SR)
The SR surrounds myofibrils and stores calcium. Upon stimulation, calcium is released into the sarcoplasm, initiating contraction.
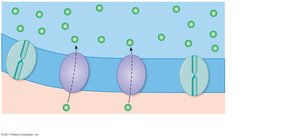
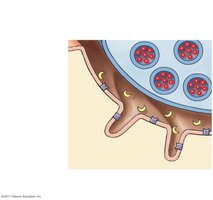
Neuromuscular Junction (NMJ)
The NMJ is the synapse between a motor neuron and a muscle fiber. Acetylcholine (ACh) is released from the neuron, binds to receptors on the motor end plate, and triggers an action potential in the muscle fiber.
Muscle Fiber Types
Classification of Skeletal Muscle Fibers
Skeletal muscle fibers are classified based on contraction speed and metabolic properties:
Fiber Type | Diameter | Contraction Speed | Fatigue Resistance | Metabolism |
|---|---|---|---|---|
Fast Twitch (Type II-B) | Large | Very fast | Low | Anaerobic |
Slow Twitch (Type I) | Small | Slow | High | Aerobic |
Intermediate (Type II-A) | Medium | Moderate | Moderate | Mixed |
Muscle Contraction Types
Isotonic and Isometric Contractions
Muscle contractions are classified by changes in muscle length:
Isotonic contraction: Muscle changes length while tension remains constant.
Concentric contraction: Muscle shortens as tension exceeds load.
Eccentric contraction: Muscle lengthens as load exceeds tension.
Isometric contraction: Muscle length does not change; tension does not exceed load.
Energy Supply and Muscle Metabolism
ATP Sources in Muscle
Muscle cells generate ATP through three main pathways:
Glycolysis: Anaerobic, occurs in sarcoplasm, produces 2 ATP per glucose.
Aerobic metabolism: Occurs in mitochondria, produces 17 ATP per pyruvate.
Creatine phosphate (CP): Stores high-energy phosphate for rapid ATP regeneration.
Equation for creatine phosphate reaction:
Muscle Fatigue and Recovery
Fatigue occurs when ATP demand exceeds supply, leading to lactic acid accumulation and decreased pH. Recovery involves conversion of lactate to pyruvate and glucose (Cori cycle), replenishing glycogen reserves, and restoring normal conditions. Oxygen debt (EPOC) is the extra oxygen required post-exercise.
Clinical Conditions Affecting Muscles
Hypertrophy and Atrophy
Hypertrophy: Increase in muscle size due to repeated stimulation, increased myofilaments, mitochondria, and glycogen.
Atrophy: Decrease in muscle size, tone, and power due to disuse or nerve damage.
Muscle Disorders
Polio: Viral attack on motor neurons, causing paralysis.
Tetanus: Bacterial toxin suppresses inhibition of motor neurons, causing sustained contractions.
Botulism: Bacterial toxin blocks ACh release, causing paralysis.
Myasthenia gravis: Autoimmune loss of ACh receptors, causing progressive weakness.
Rigor mortis: Post-mortem muscle contraction due to ATP depletion.
