 Back
BackSkeletal Muscle Tissue: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Skeletal Muscle Tissue
Overview of Muscle Tissue
Muscle tissue is highly specialized for contraction and is composed of elongated cells known as muscle fibers. These tissues are essential for movement, posture, and various physiological functions. There are three main types of muscle tissue: skeletal, cardiac, and smooth muscle.
Skeletal muscle: Moves the body by pulling on bones.
Cardiac muscle: Pumps blood through the circulatory system.
Smooth muscle: Moves fluids and solids along internal passageways and regulates vessel diameter.
Functions of Muscle Tissue
Skeletal Movement: Muscles contract and pull on tendons attached to bones, producing movement.
Maintain Posture: Continuous muscle contractions maintain body posture.
Support Soft Tissue: Skeletal muscles form the abdominal wall and pelvic floor.
Guard Entrances and Exits: Control voluntary actions such as swallowing, urination, and defecation.
Muscle Structure and Organization
Connective Tissue Layers
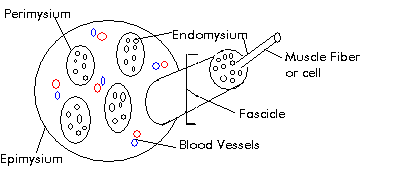
Muscle tissue is organized into several layers of connective tissue that provide structure and support:
Epimysium: Dense collagen layer that separates muscle from surrounding tissues and organs.
Perimysium: Surrounds groups of muscle fibers, forming fascicles; contains blood vessels and nerves.
Endomysium: Surrounds individual muscle fibers within a fascicle; contains capillaries and satellite cells (muscle stem cells for repair).
Anatomy of a Skeletal Muscle Fiber
Sarcolemma: The plasma membrane of a muscle fiber, responsible for conducting electrical impulses.
Sarcoplasm: The cytoplasm of a muscle fiber, containing myoglobin for oxygen storage.
Transverse (T) Tubules: Extensions of the sarcolemma that transmit action potentials deep into the muscle fiber.
Myofibrils: Cylindrical structures within muscle fibers, composed of repeating contractile units called sarcomeres.
Sarcoplasmic Reticulum (SR): Specialized endoplasmic reticulum that stores and releases calcium ions (Ca2+).
Terminal Cisternae: Enlarged areas of the SR that store Ca2+ and form a triad with T tubules.
Sarcomere Structure and Muscle Contraction
Sarcomere Organization
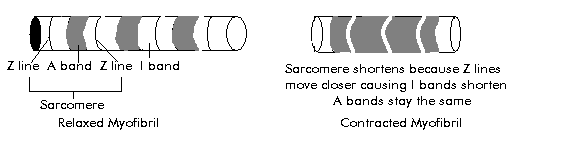
The sarcomere is the smallest functional unit of a muscle fiber, responsible for muscle contraction. Each myofibril contains thousands of sarcomeres arranged end-to-end.
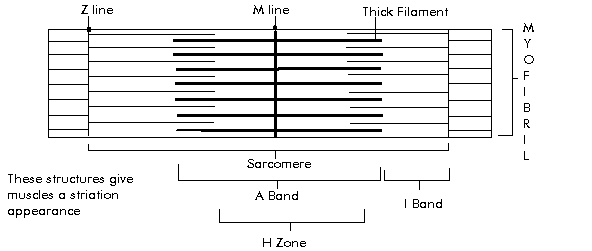
A Band: Region containing thick filaments (myosin); includes the M line and H zone.
M Line: Center of the A band; stabilizes thick filaments.
H Zone: Lighter region in the center of the A band; only thick filaments present when muscle is relaxed.
I Band: Region containing only thin filaments (actin); spans from the A band of one sarcomere to the next.
Z Line: Defines the boundaries of each sarcomere; anchors thin filaments.
Thick and Thin Filaments
Thick Filaments: Composed of myosin molecules, each with a globular head that binds to actin during contraction.
Thin Filaments: Composed of actin, tropomyosin, troponin, and nebulin. Actin contains binding sites for myosin heads.
Tropomyosin: Covers myosin-binding sites on actin, preventing contraction in the absence of Ca2+.
Troponin: Binds to Ca2+ and moves tropomyosin away from binding sites, allowing contraction.
Dystrophin: Connects actin to the endomysium, transmitting tension to the tendon.
Sliding Filament Theory
Muscle contraction occurs when thin filaments slide past thick filaments, shortening the sarcomere. This process is regulated by the presence of Ca2+ and ATP.
Ca2+ binds to troponin, causing tropomyosin to move and expose myosin-binding sites on actin.
Myosin heads bind to actin, forming cross-bridges and pulling the thin filaments toward the center of the sarcomere.
ATP is required for myosin head detachment and re-cocking for another cycle.
Neuromuscular Junction and Muscle Contraction
Neuromuscular Junction (NMJ)
The NMJ is the site where a motor neuron communicates with a muscle fiber to initiate contraction.
Synaptic Terminal: Contains synaptic vesicles filled with the neurotransmitter acetylcholine (ACh).
Synaptic Cleft: The gap between the neuron and muscle fiber.
Motor End Plate: Region of the muscle fiber's sarcolemma with ACh receptors.
Acetylcholinesterase: Enzyme that breaks down ACh, terminating the signal.
Steps of Muscle Contraction
An action potential arrives at the synaptic terminal, causing ACh release.
ACh binds to receptors on the motor end plate, changing membrane permeability and generating an action potential in the sarcolemma.
The action potential travels along T tubules, triggering Ca2+ release from the SR.
Ca2+ binds to troponin, initiating the sliding filament mechanism and muscle contraction.
Muscle Relaxation
Stimulation at the NMJ ceases, Ca2+ is pumped back into the SR, and troponin-tropomyosin complex covers actin binding sites.
Muscle returns to resting length via elastic forces, opposing muscle contractions, and gravity.
Muscle Contraction Types and Tension
All-or-None Principle
A muscle fiber contracts completely or not at all when stimulated above threshold.
Factors Affecting Tension
Resting Length: Optimal sarcomere length allows maximal tension generation.
Frequency of Stimulation: Increased frequency leads to greater tension (summation).
Twitch, Treppe, and Tetanus
Twitch: A single contraction-relaxation cycle in a muscle fiber.
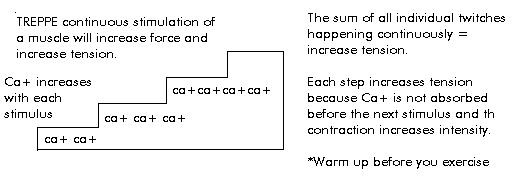
Treppe: Gradual increase in contraction strength with repeated stimulation due to incomplete Ca2+ reuptake.
Wave Summation: Successive stimuli before relaxation increase contraction strength.
Incomplete Tetanus: Muscle partially relaxes between stimuli.
Complete Tetanus: No relaxation between stimuli; maximal sustained contraction.
Motor Units and Recruitment
Motor Unit: A motor neuron and all the muscle fibers it controls.
Recruitment: Increasing the number of active motor units to increase muscle tension.
Muscle Tone: Resting tension in muscle, important for posture and shock absorption.
Types of Muscle Contraction
Isotonic Contraction: Muscle changes length (concentric: shortens; eccentric: lengthens).
Isometric Contraction: Muscle length remains the same while tension increases.
Muscle Metabolism and Energy Systems
ATP Production in Muscle
Muscle contraction requires large amounts of ATP, which is generated through three main metabolic pathways:
Direct Phosphorylation: Creatine phosphate donates a phosphate to ADP to form ATP, catalyzed by creatine kinase.
Aerobic Respiration: Glucose is broken down with oxygen in mitochondria, producing CO2, H2O, and large amounts of ATP.
Anaerobic Respiration (Glycolysis): Glucose is broken down without oxygen, producing lactic acid and small amounts of ATP.
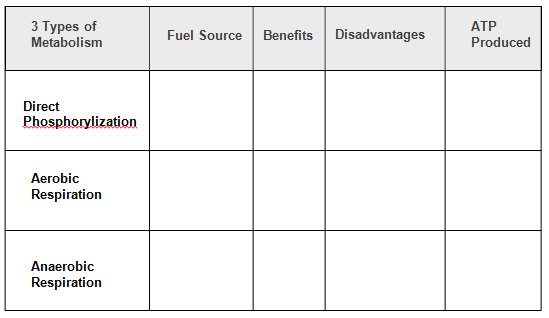
3 Types of Metabolism | Fuel Source | Benefits | Disadvantages | ATP Produced |
|---|---|---|---|---|
Direct Phosphorylization | Creatine phosphate | Rapid ATP production; immediate energy | Short duration (about 15 seconds); limited supply | 1 ATP per creatine phosphate |
Aerobic Respiration | Glucose, fatty acids, O2 | Efficient; supports prolonged activity; 36 ATP per glucose | Slow; requires oxygen; produces CO2 | ~36 ATP per glucose |
Anaerobic Respiration | Glucose | Fast; does not require oxygen; supports short bursts | Low yield (2 ATP per glucose); lactic acid buildup causes fatigue | 2 ATP per glucose |
Muscle Fatigue and Oxygen Debt
Muscle Fatigue: Inability to maintain required power output due to depletion of energy reserves, oxygen, or pH imbalance.
Oxygen Debt: Extra oxygen required after exercise to restore ATP, creatine phosphate, and glycogen levels.
Muscle Fiber Types
Classification of Muscle Fibers
Fast Fibers (Type IIa): Large diameter, rapid contraction, fatigue quickly, rely on anaerobic metabolism.
Slow Fibers (Type I): Smaller diameter, slower contraction, resist fatigue, high myoglobin content, rely on aerobic metabolism.
Intermediate Fibers (Type IIb): Characteristics between fast and slow fibers; moderate resistance to fatigue.
Muscle Adaptation and Clinical Considerations
Hypertrophy and Atrophy
Hypertrophy: Increase in muscle fiber size due to increased stimulation, more mitochondria, and greater glycogen reserves.
Atrophy: Decrease in muscle size due to lack of stimulation; can be reversible if addressed early.
Clinical Disorders
Botulism: Toxin prevents ACh release, causing paralysis.
Myasthenia Gravis: Autoimmune attack on ACh receptors, leading to muscle weakness.
Polio: Viral attack on motor neurons, causing paralysis.
Muscular Dystrophy: Genetic disorder causing muscle degeneration due to lack of dystrophin.
Cardiac and Smooth Muscle Tissue
Cardiac Muscle
Found only in the heart; striated with intercalated discs for synchronized contraction.
Single nucleus per cell; relies on aerobic metabolism; automaticity via pacemaker cells.
Smooth Muscle
Found in walls of hollow organs; non-striated; single central nucleus.
Contracts via calmodulin and myosin light chain kinase; can contract over greater lengths than skeletal muscle.
Controlled by nerves (multiunit) or involuntarily (visceral); responsible for peristalsis and regulation of vessel diameter.
