 Back
BackThe Endocrine System: Structure, Function, and Clinical Aspects
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 16: The Endocrine System
16.1 Endocrine System Overview
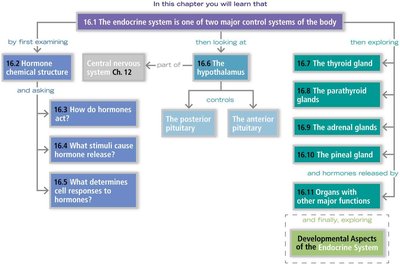
The endocrine system is one of the two major control systems of the body, working alongside the nervous system to maintain homeostasis. It influences metabolic activities through hormones transported in the blood, producing slower but longer-lasting responses compared to the nervous system. The study of hormones and endocrine organs is called endocrinology.
Major functions: Reproduction, growth and development, maintenance of electrolyte, water, and nutrient balance, regulation of cellular metabolism and energy balance, and mobilization of body defenses.
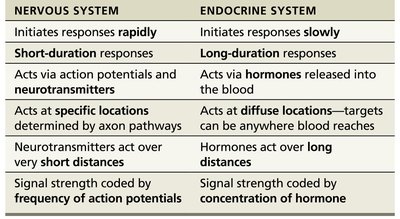
Comparison with nervous system: The nervous system initiates rapid, short-duration responses via neurotransmitters and action potentials, while the endocrine system initiates slower, long-duration responses via hormones released into the blood.
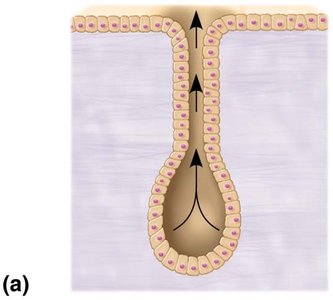
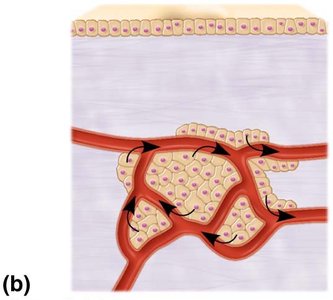
Endocrine vs. Exocrine Glands
Exocrine glands: Produce nonhormonal substances (e.g., sweat, saliva) and have ducts to carry secretions to membrane surfaces.
Endocrine glands: Produce hormones, lack ducts, and release hormones into surrounding tissues, typically with rich vascular and lymphatic drainage.
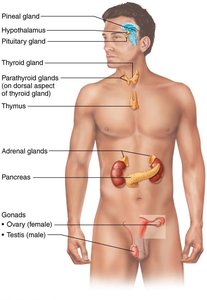
Major Endocrine Organs
Pituitary, thyroid, parathyroid, adrenal, and pineal glands
Hypothalamus (neuroendocrine organ)
Other organs with endocrine tissue: pancreas, gonads, placenta, adipose cells, thymus, and cells in the walls of the small intestine, stomach, kidneys, and heart
Chemical Messengers of the Endocrine System
Hormones: Long-distance chemical signals traveling in blood or lymph.
Autocrines: Chemicals that exert effects on the same cells that secrete them (local effect).
Paracrines: Locally acting chemicals that affect other cell types (local effect).
Autocrines and paracrines are not considered part of the endocrine system.
16.2 Hormonal Chemical Structure
Amino acid–based hormones: Includes amino acid derivatives, peptides, and proteins.
Steroid hormones: Synthesized from cholesterol; includes gonadal and adrenocortical hormones.
16.3 How Hormones Act
Hormones affect only target cells with specific receptors. Their actions include altering membrane permeability, stimulating protein synthesis, activating/deactivating enzymes, inducing secretory activity, and stimulating mitosis.
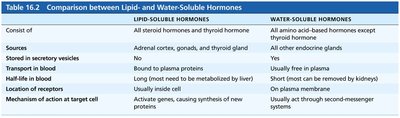
Water-soluble hormones: (All amino acid–based except thyroid hormone) Act on plasma membrane receptors, activate second messengers, and cannot enter the cell.
Lipid-soluble hormones: (Steroid and thyroid hormones) Act on intracellular receptors, directly activate genes, and can enter the cell.
Second Messenger Systems
Water-soluble hormones bind to plasma membrane receptors, triggering second messenger cascades (such as cAMP), leading to amplification of the signal.
Direct Gene Activation
Lipid-soluble hormones diffuse into target cells, bind to intracellular receptors, and initiate DNA transcription to produce mRNA, which is translated into proteins.
16.4 Hormone Release
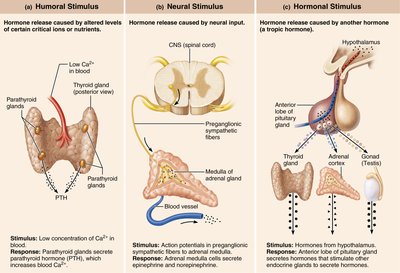
Blood levels of hormones are controlled by negative feedback systems, maintaining levels within a narrow range. Hormone release is triggered by:
Humoral stimuli: Changes in blood levels of ions or nutrients.
Neural stimuli: Nerve fibers stimulate hormone release.
Hormonal stimuli: Hormones stimulate other endocrine glands to release hormones.
Nervous System Modulation
The nervous system can override normal endocrine controls, especially during stress (e.g., fight or flight response).
Transport and Half-Life of Hormones
Lipid-soluble hormones are bound to plasma proteins; water-soluble hormones circulate freely.
Half-life is the time required for hormone blood level to decrease by half; shortest for water-soluble hormones.
Hormone Interactions at Target Cells
Permissiveness: One hormone cannot exert its effects without another hormone present.
Synergism: More than one hormone produces the same effect, amplifying the response.
Antagonism: One or more hormones oppose the action of another hormone.
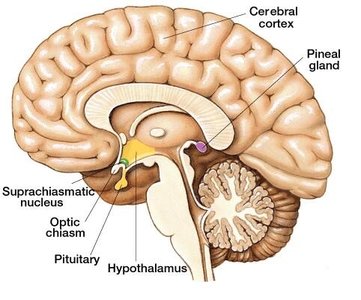
16.6 The Hypothalamus and Pituitary Gland
The hypothalamus is a neuroendocrine organ that controls the release of hormones from the pituitary gland via neural and vascular connections. The pituitary gland has two lobes: the posterior pituitary (neural tissue) and the anterior pituitary (glandular tissue).
Posterior pituitary: Stores and releases oxytocin and antidiuretic hormone (ADH) produced by the hypothalamus.
Anterior pituitary: Produces and releases six peptide hormones, most of which are tropic (regulate other endocrine glands).

Posterior Pituitary Hormones
Oxytocin: Stimulates uterine contractions during childbirth and milk ejection during breastfeeding; acts via positive feedback.
Antidiuretic hormone (ADH): Promotes water reabsorption in kidneys, reducing urine output; inhibited by alcohol and diuretics.
Clinical Correlates
Diabetes insipidus: Hyposecretion of ADH, causing excessive urine output and thirst.
SIADH: Hypersecretion of ADH, leading to fluid retention and hyponatremia.
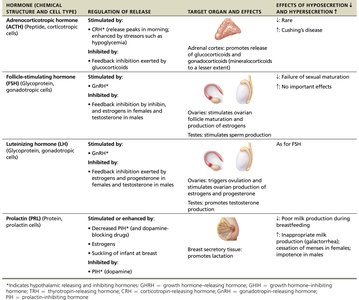
Anterior Pituitary Hormones
Growth hormone (GH): Stimulates growth via insulin-like growth factors (IGFs); regulated by GHRH and GHIH from the hypothalamus.
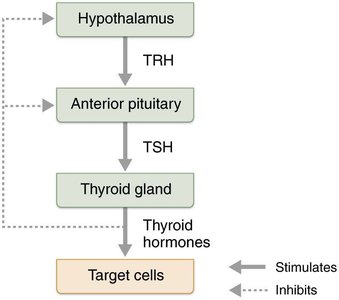
Thyroid-stimulating hormone (TSH): Stimulates thyroid gland; regulated by TRH from the hypothalamus.
Adrenocorticotropic hormone (ACTH): Stimulates adrenal cortex; regulated by CRH from the hypothalamus.
Follicle-stimulating hormone (FSH) and Luteinizing hormone (LH): Regulate gonadal function; controlled by GnRH.
Prolactin (PRL): Stimulates milk production; regulated by PIH (dopamine).
16.7 The Thyroid Gland
The thyroid gland is a butterfly-shaped organ located in the anterior neck, consisting of follicles (site of thyroid hormone production) and parafollicular cells (produce calcitonin).
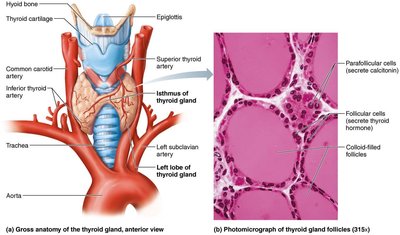
Thyroid Hormone (TH)
Major metabolic hormone, found as T4 (thyroxine) and T3 (triiodothyronine).
Increases basal metabolic rate, regulates tissue growth and development, and maintains blood pressure.
Regulated by negative feedback involving TSH and TRH.
Clinical Correlates
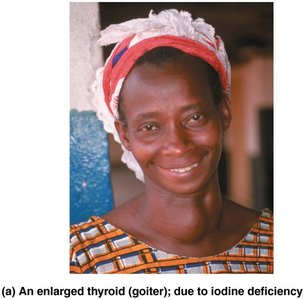
Hyposecretion (myxedema): Low metabolic rate, chills, edema; goiter if due to iodine deficiency.
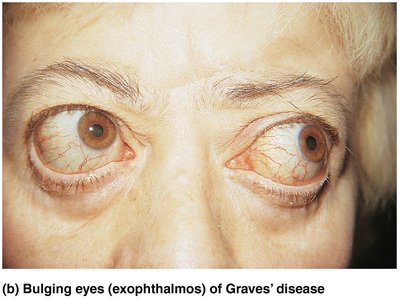
Hypersecretion (Graves' disease): Elevated metabolic rate, weight loss, exophthalmos (bulging eyes).
Calcitonin
Produced by parafollicular cells in response to high Ca2+ levels; antagonizes parathyroid hormone (PTH).
At pharmacological doses, inhibits osteoclast activity and stimulates Ca2+ uptake into bone.
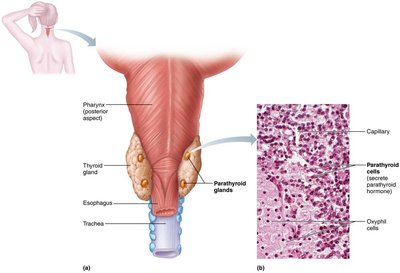
16.8 The Parathyroid Glands
Four to eight small glands on the posterior thyroid, secreting parathyroid hormone (PTH), the most important hormone in Ca2+ homeostasis.
Stimulates osteoclasts, enhances Ca2+ reabsorption by kidneys, and promotes vitamin D activation for increased intestinal absorption.

Clinical Correlates
Hyperparathyroidism: Bone softening, kidney stones, nervous system depression.
Hypoparathyroidism: Tetany, respiratory paralysis, and potentially death.
16.9 The Adrenal Glands
Paired glands atop the kidneys, consisting of the adrenal cortex (three layers producing corticosteroids) and the adrenal medulla (producing catecholamines).
Zona glomerulosa: Mineralocorticoids (e.g., aldosterone) regulate Na+ and K+ balance.
Zona fasciculata: Glucocorticoids (e.g., cortisol) regulate metabolism and stress response.
Zona reticularis: Gonadocorticoids (weak androgens).

Adrenal Medulla
Produces epinephrine and norepinephrine, reinforcing the fight-or-flight response.
Effects: Vasoconstriction, increased heart rate, increased blood glucose, blood flow to brain/heart/muscle.
The Stress Response
Short-term stress: SNS and adrenal medulla (catecholamines).
Long-term stress: Adrenal cortex (corticosteroids), leading to increased ACTH, cortisol, and aldosterone.
Exhaustion: Prolonged stress disrupts homeostasis, causing hypertension, muscle loss, immune suppression, etc.
16.10 The Pineal Gland
Small gland in the brain that secretes melatonin, regulating sleep-wake cycles and acting as an antioxidant.
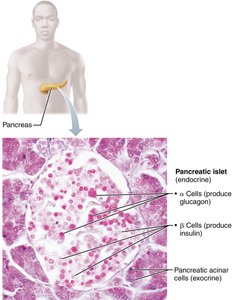
16.11 The Pancreas
The pancreas has both exocrine (digestive enzymes) and endocrine (hormones) functions. The pancreatic islets contain alpha cells (glucagon) and beta cells (insulin).
Glucagon: Raises blood glucose by promoting glycogen breakdown and gluconeogenesis in the liver.
Insulin: Lowers blood glucose by enhancing cellular uptake and storage as glycogen, and inhibiting gluconeogenesis.

Clinical Correlates
Diabetes mellitus (DM): Hyposecretion (Type 1) or hypoactivity (Type 2) of insulin, leading to hyperglycemia, polyuria, polydipsia, and polyphagia. Long-term complications include vascular and nerve damage.
Hyperinsulinism: Excess insulin causes hypoglycemia, with symptoms such as anxiety, unconsciousness, and potentially death.

The Gonads and Placenta
Ovaries: Produce estrogens and progesterone, responsible for female reproductive organ maturation and secondary sexual characteristics.
Testes: Produce testosterone, responsible for male reproductive organ maturation, secondary sexual characteristics, and sperm production.
Placenta: Temporary endocrine organ producing estrogens, progesterone, and hCG during pregnancy.
Hormone Secretion by Other Organs
Adipose tissue: Leptin regulates appetite and energy balance.
Gastrointestinal tract: Enteroendocrine cells regulate digestion.
Heart: Atrial natriuretic peptide (ANP) decreases blood pressure.
Kidneys: Erythropoietin stimulates red blood cell production; renin regulates blood pressure.
Skeleton: Osteocalcin influences insulin secretion and fat storage.
Skin: Produces cholecalciferol (vitamin D precursor).
Thymus: Involved in T lymphocyte development and immune response.
Developmental Aspects of the Endocrine System
Most endocrine organs function well until old age, but GH and TH levels decline, contributing to muscle atrophy and lower metabolic rates.
PTH levels remain constant, but postmenopausal women are more vulnerable to bone loss due to decreased estrogen.
Glucose tolerance deteriorates with age.
