 Back
BackThe Endocrine System: Thyroid, Parathyroid, Adrenal, Pineal, Pancreas, and Other Endocrine Organs
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Endocrine System
Overview
The endocrine system is a collection of glands that secrete hormones directly into the bloodstream to regulate various physiological processes. This section focuses on the thyroid, parathyroid, adrenal, pineal glands, pancreas, and other hormone-secreting organs, emphasizing their structure, function, regulation, and clinical significance.
The Thyroid Gland
Location and Structure
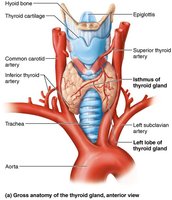
The thyroid gland is a butterfly-shaped organ located in the anterior neck, just inferior to the larynx and overlaying the trachea. It consists of two lateral lobes connected by a median mass called the isthmus. The gland is composed of follicles, which are hollow spheres of epithelial follicular cells that produce the glycoprotein thyroglobulin. The lumen of these follicles contains colloid, a fluid rich in thyroglobulin and iodine, serving as the precursor to thyroid hormone. Parafollicular cells, found between the follicles, produce the hormone calcitonin.

Thyroid Hormone (TH)
Thyroid hormone is the body's major metabolic hormone and exists in two forms: T4 (thyroxine) and T3 (triiodothyronine). T4 contains four iodine atoms, while T3 contains three. T4 is the predominant form secreted by the thyroid, but T3 is more active and is produced at the tissue level by conversion from T4. Both are iodine-containing amine hormones.
Functions:
Increases basal metabolic rate and heat production (calorigenic effect)
Regulates tissue growth and development, especially for the skeletal and nervous systems and reproductive capabilities
Maintains blood pressure by increasing adrenergic receptors in blood vessels
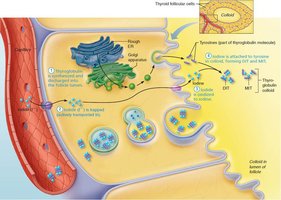
Synthesis of Thyroid Hormone
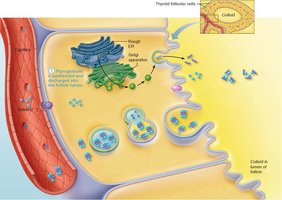
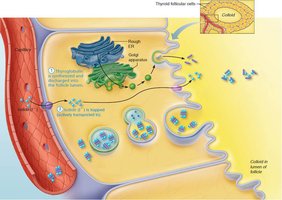
The synthesis of thyroid hormone involves several steps, primarily occurring in the follicular cells and the colloid of the thyroid gland:
Thyroglobulin is synthesized and secreted into the follicle lumen.
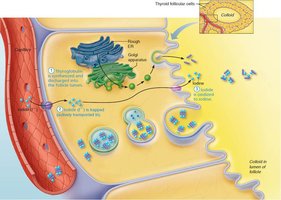
Iodide ions (I–) are actively transported into the cell and released into the lumen.
Iodide is oxidized to iodine (I2).
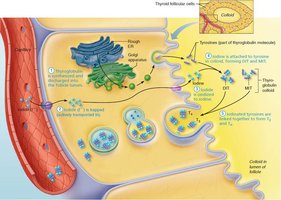
Iodine is attached to tyrosine residues on thyroglobulin, forming monoiodotyrosine (MIT) and diiodotyrosine (DIT).
Iodinated tyrosines are linked to form T3 (MIT + DIT) and T4 (DIT + DIT).
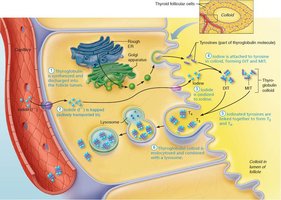
Colloid is endocytosed by follicular cells and combined with lysosomes.
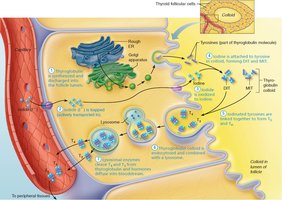
Lysosomal enzymes cleave T3 and T4 from thyroglobulin, releasing them into the bloodstream.
Transport and Regulation of Thyroid Hormone
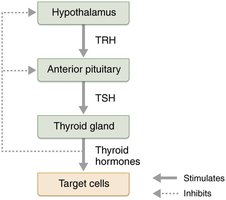
T4 and T3 are transported in the blood by thyroxine-binding globulins (TBGs). T3 is about ten times more active than T4. Peripheral tissues convert T4 to T3 by removing one iodine atom. The release of thyroid hormone is regulated by negative feedback involving the hypothalamus, anterior pituitary, and thyroid gland:
Falling TH levels stimulate the release of thyroid-stimulating hormone (TSH).
Rising TH levels inhibit TSH secretion.
Other inhibitors include GHIH, dopamine, cortisol, and high iodide levels.
Thyrotropin-releasing hormone (TRH) from the hypothalamus can override negative feedback in certain conditions (e.g., pregnancy, cold exposure).
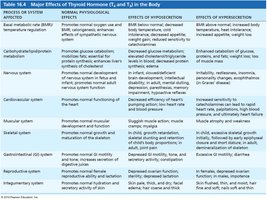
Major Effects of Thyroid Hormone
Thyroid hormones have widespread effects on various body systems. The following table summarizes their normal physiological effects and the consequences of hypo- and hypersecretion:
Process/System | Normal Effects | Effects of Hyposecretion | Effects of Hypersecretion |
|---|---|---|---|
Basal metabolic rate/temperature regulation | Promotes normal oxygen use and BMR; increases heat production | BMR below normal; decreased body temperature; cold intolerance | BMR above normal; increased body temperature; heat intolerance |
Carbohydrate/lipid/protein metabolism | Promotes glucose catabolism; enhances cholesterol synthesis and clearance | Decreased glucose metabolism; elevated cholesterol/triglycerides | Enhanced glucose catabolism; decreased cholesterol/triglycerides |
Nervous system | Promotes normal development and function | Infant: mental retardation; Adult: depression, memory impairment | Irritability, restlessness, insomnia |
Cardiovascular system | Promotes normal heart function | Decreased heart rate, low output | Increased heart rate, high output |
Muscular system | Promotes normal muscle development and function | Weak, sluggish muscles | Muscle atrophy, weakness |
Skeletal system | Promotes normal growth and maturation of skeleton | Impaired growth, delayed bone maturation | Accelerated growth, early closure of epiphyseal plates |
Gastrointestinal system | Promotes normal GI motility and tone | Decreased motility, constipation | Increased motility, diarrhea |
Reproductive system | Promotes normal reproductive function | Impaired fertility, menstrual irregularities | Menstrual irregularities, decreased fertility |
Integumentary system | Promotes normal hydration and secretion of skin | Pale, thick, dry skin; hair loss | Flushed, moist skin; thin hair |
Clinical Correlations: Thyroid Disorders
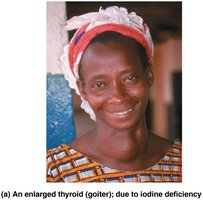
Hyposecretion (Myxedema): Low metabolic rate, dry skin, puffy eyes, lethargy. If due to iodine deficiency, a goiter (enlarged thyroid) may develop.
Congenital Hypothyroidism: In infants, it leads to impaired growth and brain development. Early treatment with TH replacement is crucial.
Hypersecretion (Graves' Disease): Autoimmune disorder causing elevated metabolic rate, weight loss, nervousness, and exophthalmos (protruding eyes).

Calcitonin
Calcitonin is produced by parafollicular (C) cells in response to high blood calcium levels. It acts as an antagonist to parathyroid hormone (PTH) by inhibiting osteoclast activity and stimulating calcium uptake into bone. Its physiological role in humans is minimal at normal levels but becomes significant at pharmacological doses.
The Parathyroid Glands
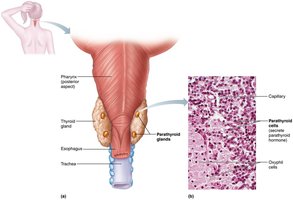
Structure and Function
The parathyroid glands are small, yellow-brown glands located on the posterior aspect of the thyroid gland. They contain parathyroid cells that secrete parathyroid hormone (PTH), the most important hormone in calcium homeostasis. PTH is secreted in response to low blood calcium and acts on the skeleton, kidneys, and intestine to increase blood calcium levels.
Actions of Parathyroid Hormone
Stimulates osteoclasts to digest bone matrix and release calcium into the blood
Enhances reabsorption of calcium and excretion of phosphate by the kidneys
Promotes activation of vitamin D by the kidneys, increasing intestinal absorption of calcium

Clinical Correlations: Parathyroid Disorders
Hyperparathyroidism: Usually due to a tumor; causes bone softening, kidney stones, and nervous system depression.
Hypoparathyroidism: Often follows gland trauma or removal; leads to hypocalcemia, tetany, respiratory paralysis, and can be fatal if untreated.
The Adrenal Glands
Structure
The adrenal glands are paired, pyramid-shaped organs atop the kidneys. Each gland consists of two regions: the adrenal cortex (glandular tissue) and the adrenal medulla (nervous tissue). The cortex produces corticosteroids, while the medulla produces catecholamines.
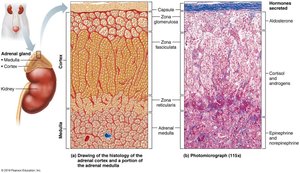
Adrenal Cortex
Zona glomerulosa: Produces mineralocorticoids (e.g., aldosterone)
Zona fasciculata: Produces glucocorticoids (e.g., cortisol)
Zona reticularis: Produces gonadocorticoids (e.g., androgens)
Mineralocorticoids (Aldosterone)
Regulate electrolyte balance, especially sodium and potassium. Aldosterone increases sodium reabsorption and potassium excretion by the kidneys, affecting blood volume and pressure. Its secretion is regulated by the renin-angiotensin-aldosterone mechanism, plasma potassium levels, ACTH, and atrial natriuretic peptide (ANP).

Glucocorticoids (Cortisol)
Influence metabolism, help resist stress, and maintain blood glucose and pressure. Cortisol promotes gluconeogenesis, mobilizes fats, and suppresses inflammation and immune responses. Its secretion is regulated by ACTH and negative feedback.
Gonadocorticoids
Weak androgens that contribute to puberty, secondary sex characteristics, and female sex drive. In postmenopausal women, they are a source of estrogens.
Adrenal Medulla
Composed of chromaffin cells that secrete catecholamines (epinephrine and norepinephrine). These hormones mediate the fight-or-flight response, increasing heart rate, blood pressure, and blood glucose, and diverting blood to essential organs.
Clinical Correlations: Adrenal Disorders
Aldosteronism: Hypersecretion of aldosterone causes hypertension and hypokalemia.
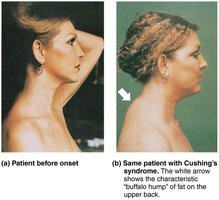
Cushing's Syndrome: Excess glucocorticoids cause muscle and bone loss, immune suppression, and characteristic fat redistribution ("moon face," "buffalo hump").
Addison's Disease: Deficits in glucocorticoids and mineralocorticoids cause weight loss, dehydration, hypotension, and skin bronzing.
Adrenogenital Syndrome: Excess androgens cause masculinization in females and precocious puberty in boys.
Pheochromocytoma: Tumor of the adrenal medulla causing excessive catecholamine secretion and sympathetic overactivity.
The Pineal Gland
Structure and Function
The pineal gland is a small structure hanging from the roof of the third ventricle. Pinealocytes secrete melatonin, which regulates circadian rhythms, sexual maturation, and may have antioxidant properties.
The Pancreas
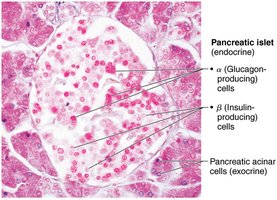
Structure and Function
The pancreas is a triangular gland with both exocrine (acinar cells) and endocrine (islets of Langerhans) functions. Alpha cells secrete glucagon (raises blood glucose), and beta cells secrete insulin (lowers blood glucose).
Glucagon
Glucagon is a potent hyperglycemic agent, raising blood glucose by promoting glycogenolysis and gluconeogenesis in the liver.
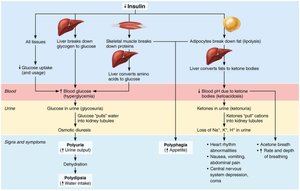
Insulin
Insulin lowers blood glucose by enhancing cellular uptake, inhibiting glycogen breakdown, and preventing gluconeogenesis. It also promotes fat and protein synthesis.

Clinical Correlations: Pancreatic Disorders
Diabetes Mellitus (DM): Due to insulin deficiency (Type 1) or resistance (Type 2). Characterized by polyuria, polydipsia, and polyphagia. Untreated DM leads to lipidemia, ketoacidosis, and severe complications.
Hyperinsulinism: Excess insulin causes hypoglycemia, which can lead to nervous system dysfunction and death if untreated.
The Gonads and Placenta
Ovaries
Ovaries produce estrogens and progesterone, responsible for female reproductive organ maturation, secondary sexual characteristics, and menstrual cycle regulation.
Testes
Testes produce testosterone, which initiates male reproductive organ development, secondary sexual characteristics, and maintains sperm production and sex drive.
Placenta
The placenta secretes estrogens, progesterone, and human chorionic gonadotropin (hCG) during pregnancy.
Other Hormone-Secreting Organs
Adipose tissue: Leptin (appetite control), resistin (insulin antagonist), adiponectin (enhances insulin sensitivity)
Gastrointestinal tract: Gastrin, ghrelin, secretin, cholecystokinin, incretins
Heart: Atrial natriuretic peptide (ANP) lowers blood pressure
Kidneys: Erythropoietin (RBC production), renin (RAA mechanism)
Skeleton: Osteocalcin (regulates insulin and fat storage)
Skin: Cholecalciferol (vitamin D precursor), calcitriol (active vitamin D)
Thymus: Thymulin, thymopoietins, thymosins (T cell development)
Developmental Aspects of the Endocrine System
Hormone-producing glands arise from all three germ layers.
Environmental pollutants can disrupt hormone function, affecting sex hormones, thyroid hormone, and glucocorticoids.
Endocrine function generally declines with age, especially GH and TH, contributing to muscle atrophy and lower metabolic rates. Ovarian and testicular function also diminish with age.
