 Back
BackThe Heart: Structure, Function, and Cardiac Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Heart: Structure, Function, and Cardiac Physiology
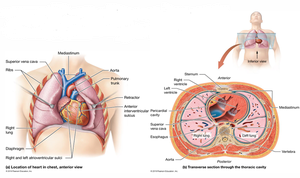
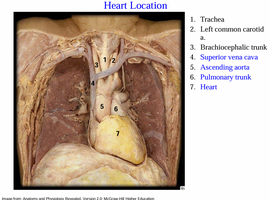
Heart Location and Orientation
The heart is located in the anterior mediastinum, directly posterior to the sternum, with its apex pointing left of the midline. The base of the heart is where the "great vessels" are attached. Understanding the anatomical position is crucial for clinical assessment and procedures.
Anterior mediastinum: Central compartment of the thoracic cavity.
Apex: Points leftward, important for auscultation and imaging.
Base: Attachment site for major vessels (aorta, pulmonary trunk).
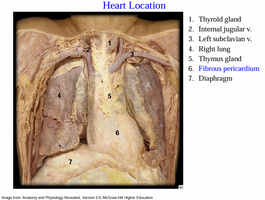
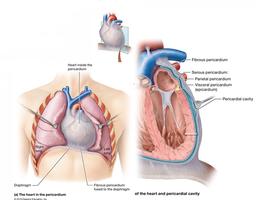
Pericardium
The pericardium is a double-layered sac that surrounds and protects the heart. It is anchored to the diaphragm and great vessels, providing structural support and reducing friction during heart movements.
Fibrous pericardium: Dense irregular connective tissue, anchors heart.
Serous pericardium: Two layers—parietal (lines sac) and visceral (epicardium, covers heart).
Pericardial cavity: Space between layers, filled with pericardial fluid for lubrication.
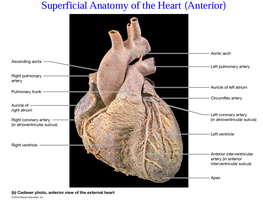
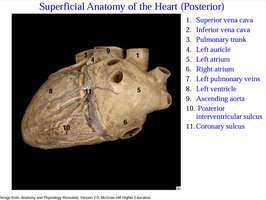
Superficial Anatomy of the Heart
The heart's external features include sulci and major vessels. The atrioventricular sulcus separates the atria from the ventricles, while the interventricular sulcus overlies the septum dividing the right and left ventricles. These sulci contain coronary arteries, which supply the heart muscle.
Atrioventricular sulcus: Boundary between atria and ventricles.
Interventricular sulcus: Marks the septum between ventricles.
Coronary arteries: Located within sulci, essential for myocardial perfusion.
Heart Wall Structure
The heart wall is composed of three distinct layers, each with specialized functions:
Epicardium (visceral pericardium): Outermost layer, provides protection.
Myocardium: Middle layer, consists of concentric cardiac muscle tissue (myocytes), blood vessels, and nerves. The fibrous skeleton provides structural support, anchors myocytes, prevents over-expansion, and maintains elasticity.
Endocardium: Innermost layer, simple squamous epithelium lining chambers and valves, continuous with endothelium of great vessels.
Example: The myocardium is much thicker in the left ventricle than the right, reflecting its role in generating higher pressure for systemic circulation.
Blood Flow Through the Heart
Blood flows through the heart in a specific sequence, regulated by valves and septa:
Right Atrium (RA): Receives blood from superior/inferior vena cava and coronary sinus; separated from left atrium by interatrial septum (fossa ovalis).
Right Ventricle (RV): Receives blood via tricuspid valve; thinner wall than LV; ejects blood into pulmonary trunk via pulmonary semilunar valve.
Left Atrium (LA): Receives oxygenated blood from pulmonary veins; sends blood to LV via bicuspid (mitral) valve.
Left Ventricle (LV): Thickest wall; ejects blood into aorta via aortic semilunar valve.
Formula: Stroke Volume (SV) = End-Diastolic Volume (EDV) − End-Systolic Volume (ESV)
Example: If EDV = 120 mL and ESV = 50 mL, then SV = 70 mL.
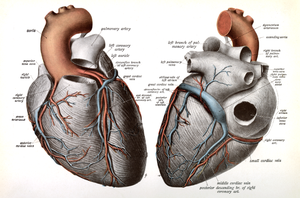
Coronary Circulation
The heart's own blood supply is provided by the coronary arteries and veins. Coronary circulation is essential for myocardial function and is characterized by extensive anastomoses.
Right coronary artery: Supplies RA and RV via marginal and posterior interventricular arteries.
Left coronary artery: Supplies LV and LA via left anterior descending (LAD) and circumflex arteries.
Coronary sinus: Major venous drainage into RA; receives blood from great, small, and middle cardiac veins.
Anastomoses: Interconnections ensure continuous blood flow.
Cardiac Muscle Tissue and Metabolism
Cardiac myocytes are specialized for endurance and efficient contraction. Intercalated discs, desmosomes, and gap junctions facilitate force transmission and rapid electrical propagation.
Intercalated discs: Contain desmosomes (mechanical anchors) and gap junctions (electrical synapses).
Myocyte characteristics: Small, single nucleus, branching, high myoglobin and mitochondria content.
Metabolism: Relies on aerobic respiration; uses fatty acids, glucose, lactate; highly fatigue-resistant.
Comparison: Cardiac muscle is more fatigue-resistant than skeletal muscle due to its reliance on aerobic metabolism and abundant mitochondria.
Cardiac Electrophysiology and Conduction System
The heart's electrical system coordinates contraction through specialized conducting cells and pathways. The heart acts as a functional syncytium, allowing coordinated contraction.
Contractile cells: Produce muscular contraction upon depolarization.
Conducting cells: Generate and propagate electrical impulses; include SA node, AV node, bundle branches, Purkinje fibers.
SA node: Pacemaker, initiates heartbeat, sets heart rate.
AV node: Electrical gateway to ventricles; delays signal for proper timing.
Bundle of His and Purkinje fibers: Rapidly distribute signal to ventricular myocardium.
HCN channels: Hyperpolarization-activated cyclic nucleotide-gated channels in pacemaker cells generate the "funny current" (If), crucial for spontaneous depolarization and heart rate regulation.
Electrocardiography (ECG/EKG)
ECG is a diagnostic tool for assessing heart function, conduction pathways, and detecting abnormalities such as myocardial infarction, nodal damage, and electrolyte imbalances.
ECG: Records electrical activity of the heart.
Diagnostic value: Identifies conduction abnormalities, heart enlargement, and more.
Excitation-Contraction Coupling in Cardiac Myocytes
Electrical signals trigger mechanical contraction in cardiac myocytes through calcium dynamics:
Extracellular Ca2+: Enters via voltage-gated channels during plateau phase.
Calcium-induced calcium release (CICR): Triggers release from sarcoplasmic reticulum.
Troponin C: Ca2+ binds, initiating contraction.
Relaxation: Ca2+ pumped back into SR and out of cell.
Cardiac Cycle and Heart Sounds
The cardiac cycle consists of alternating systole (contraction) and diastole (relaxation) phases, governed by pressure gradients and valve function. Heart sounds are produced by valve closure and blood turbulence.
S1 (lupp): Closure of AV valves at start of ventricular systole.
S2 (dupp): Closure of semilunar valves at start of ventricular diastole.
Heart murmur: Abnormal sound, may indicate valve pathology.
Cardiodynamics: Stroke Volume and Cardiac Output
Cardiac output is determined by stroke volume and heart rate. Stroke volume depends on preload, contractility, and afterload.
End-Diastolic Volume (EDV): Volume at end of diastole (~120 mL).
End-Systolic Volume (ESV): Volume after systole (~50 mL).
Stroke Volume (SV): SV = EDV − ESV.
Preload: Tension in myocardium before contraction; increased preload increases SV (Frank–Starling law).
Contractility: Force of contraction independent of preload.
Afterload: Resistance the ventricle must overcome to eject blood.
Frank–Starling Law: Stroke volume is proportional to end-diastolic volume.
Heart Rate Regulation
Heart rate is regulated by the autonomic nervous system, hormones, and ion concentrations.
Sympathetic division: Increases heart rate and contractility.
Parasympathetic division: Decreases heart rate.
Hormones: Epinephrine, norepinephrine, thyroid hormones increase heart rate.
Ions: Excess K+ decreases heart rate; excess Ca2+ increases contractility and may increase heart rate.
Summary: Factors Affecting Cardiac Output
Cardiac output is the product of stroke volume and heart rate, influenced by preload, contractility, afterload, autonomic regulation, hormones, and ion concentrations.
Cardiac Output (CO): CO = SV × HR
Key determinants: EDV, ESV, preload, contractility, afterload, autonomic input, hormones, ions.
