Back
BackThe Human Heart: Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Human Heart: Structure, Function, and Clinical Relevance
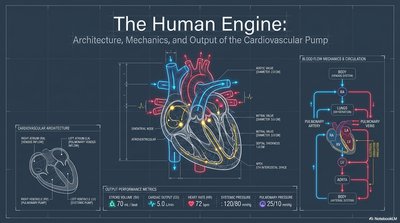
Cardiovascular Architecture and Output
The heart is a muscular organ responsible for pumping blood throughout the body, ensuring the delivery of oxygen and nutrients while removing waste products. Its architecture and mechanics are optimized for efficient circulation through two main circuits: the pulmonary and systemic circuits.
Cardiac Chambers: The heart consists of four chambers: right atrium, right ventricle, left atrium, and left ventricle.
Valves: One-way valves (tricuspid, pulmonary, mitral, aortic) prevent backflow and ensure unidirectional blood flow.
Pulmonary Circuit: Right side pumps deoxygenated blood to the lungs for oxygenation.
Systemic Circuit: Left side pumps oxygenated blood to the rest of the body.
Performance Metrics: Normal cardiac output is about 5.0 L/min, with a heart rate of ~70 bpm and stroke volume of ~70 mL.
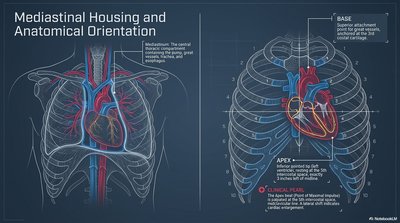
Mediastinal Housing and Anatomical Orientation
The heart is located in the mediastinum, a central thoracic compartment between the lungs. Its anatomical orientation is crucial for clinical assessment and imaging.
Base: Superior attachment point for great vessels, oriented toward the right shoulder.
Apex: Inferior, leftward tip of the heart, important for auscultation and clinical assessment.
Clinical Pearl: The apex beat (point of maximal impulse) is palpated at the 5th intercostal space, midclavicular line.
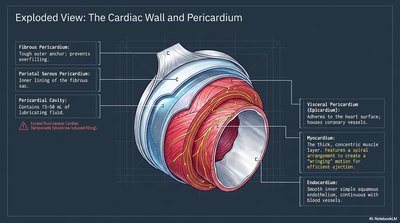
Cardiac Wall and Pericardium
The heart wall is composed of three layers, each with distinct structure and function, and is enclosed by the pericardium, which provides protection and reduces friction.
Fibrous Pericardium: Tough outer layer, prevents overfilling.
Serous Pericardium: Double-layered (parietal and visceral), with a lubricating pericardial cavity in between.
Myocardium: Thick, muscular middle layer responsible for contraction.
Endocardium: Smooth inner lining, minimizes friction and lines chambers/valves.
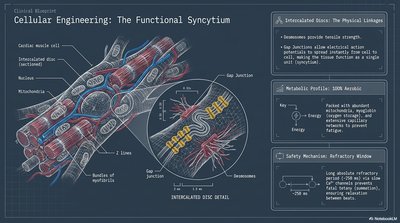
Cellular Engineering: The Functional Syncytium
Cardiac muscle cells (cardiomyocytes) are interconnected by intercalated discs, forming a functional syncytium that allows coordinated contraction.
Intercalated Discs: Contain desmosomes (mechanical strength) and gap junctions (electrical connectivity).
Metabolic Profile: Highly aerobic, abundant mitochondria for sustained contraction.
Refractory Window: Long refractory period prevents tetanus, ensuring rhythmic contractions.
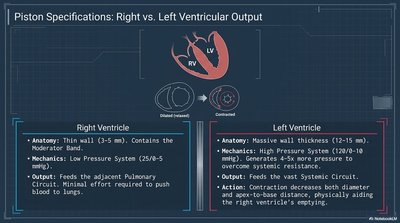
Right vs. Left Ventricular Output
The right and left ventricles have distinct anatomical and functional properties, reflecting their roles in the pulmonary and systemic circuits.
Right Ventricle | Left Ventricle |
|---|---|
Thin wall (3-5 mm), low pressure (25/5 mmHg), pumps to lungs | Thick wall (12-15 mm), high pressure (120/10 mmHg), pumps to systemic circuit |
Minimal force required | Generates 4-5x more pressure |
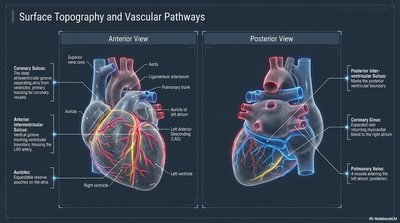
Surface Topography and Vascular Pathways
The heart's surface features and vascular pathways are essential for understanding coronary circulation and clinical interventions.
Coronary Sulcus: Encircles the heart, marking the boundary between atria and ventricles.
Coronary Arteries: Supply oxygenated blood to the myocardium.
Coronary Sinus: Collects deoxygenated blood from the myocardium and returns it to the right atrium.
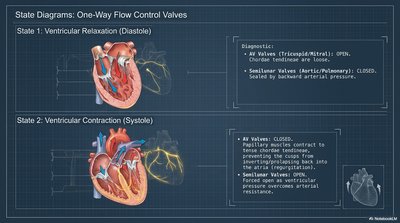
One-Way Flow Control Valves
Heart valves ensure unidirectional blood flow and prevent backflow during the cardiac cycle.
Diastole (Relaxation): AV valves (tricuspid/mitral) open, semilunar valves closed.
Systole (Contraction): AV valves closed, semilunar valves (aortic/pulmonary) open.
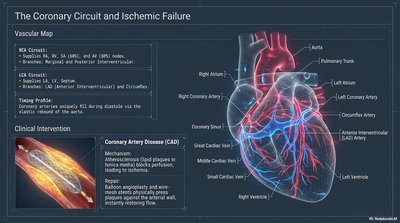
The Coronary Circuit and Ischemic Failure
The coronary arteries supply the heart muscle itself. Blockage can lead to ischemia and myocardial infarction (heart attack).
Right Coronary Artery (RCA): Supplies right atrium, ventricle, and part of septum.
Left Coronary Artery (LCA): Supplies left atrium, ventricle, and septum.
Clinical Note: Coronary artery disease (CAD) is a leading cause of morbidity and mortality.
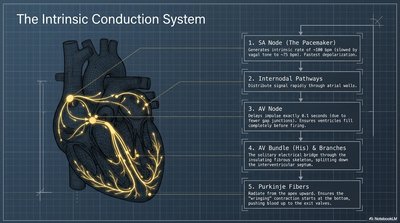
The Intrinsic Conduction System
The heart's electrical system coordinates contraction, ensuring efficient pumping.
SA Node: Pacemaker, initiates heartbeat.
AV Node: Delays impulse, allowing atrial contraction before ventricular contraction.
Bundle of His & Purkinje Fibers: Rapidly distribute impulse to ventricles.
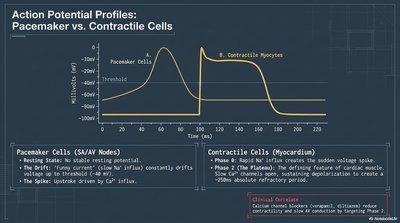
Action Potential Profiles: Pacemaker vs. Contractile Cells
Cardiac action potentials differ between pacemaker cells (SA/AV nodes) and contractile myocytes (muscle cells).
Pacemaker Cells: Unstable resting potential, spontaneous depolarization (automaticity).
Contractile Cells: Stable resting potential, rapid depolarization, plateau phase due to Ca2+ influx.
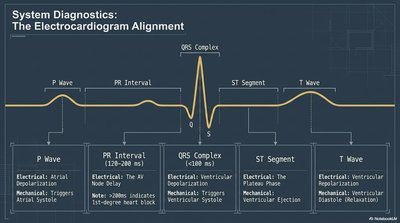
Electrocardiogram (ECG) Alignment
The ECG records the electrical activity of the heart, with distinct waves corresponding to different phases of the cardiac cycle.
Wave/Interval | Electrical Event | Mechanical Event |
|---|---|---|
P Wave | Atrial depolarization | Atrial systole |
PR Interval | AV node delay | Ventricular filling |
QRS Complex | Ventricular depolarization | Ventricular systole |
ST Segment | Plateau phase | Ventricular ejection |
T Wave | Ventricular repolarization | Ventricular diastole |
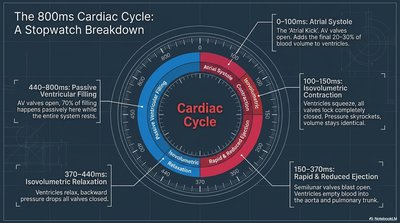
The Cardiac Cycle: Stopwatch Breakdown
The cardiac cycle consists of a sequence of events that occur during one heartbeat, typically lasting about 800 ms.
Atrial Systole (0-100 ms): Atria contract, topping off ventricular volume.
Isovolumetric Contraction (100-150 ms): Ventricles contract, all valves closed, pressure rises.
Ventricular Ejection (150-370 ms): Semilunar valves open, blood ejected.
Isovolumetric Relaxation (370-440 ms): Ventricles relax, all valves closed.
Passive Ventricular Filling (440-800 ms): AV valves open, ventricles fill.
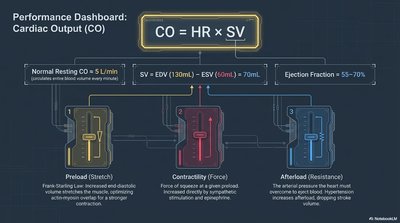
Cardiac Output (CO)
Cardiac output is the volume of blood pumped by each ventricle per minute. It is a key measure of heart performance.
Formula:
HR: Heart rate (beats per minute)
SV: Stroke volume (mL/beat)
Normal Resting CO: ~5 L/min
Determinants: Preload (stretch), contractility (force), afterload (resistance)
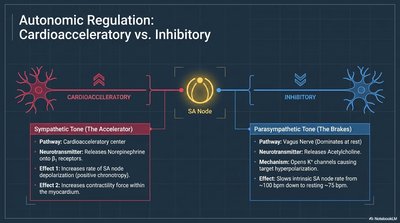
Autonomic Regulation: Cardioacceleratory vs. Inhibitory
The autonomic nervous system regulates heart rate and contractility via sympathetic and parasympathetic pathways.
Sympathetic (Cardioacceleratory): Increases heart rate and contractility via norepinephrine.
Parasympathetic (Inhibitory): Decreases heart rate via acetylcholine (vagus nerve).
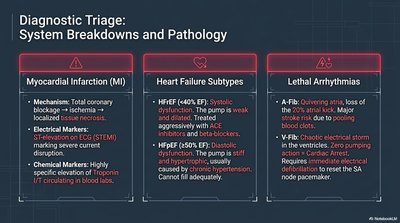
System Breakdowns and Pathology
Common cardiac pathologies include myocardial infarction, heart failure, and lethal arrhythmias.
Myocardial Infarction (MI): Blockage of coronary artery leads to ischemia and tissue necrosis. Diagnosed by ECG and elevated troponin.
Heart Failure: Systolic (HFrEF) or diastolic (HFpEF) dysfunction, often due to hypertension or ischemic injury.
Lethal Arrhythmias: Atrial fibrillation (A-Fib) and ventricular fibrillation (V-Fib) disrupt cardiac output and can be fatal without intervention.