 Back
BackThe Knee Joint: Structure, Function, and Clinical Anatomy
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Knee Joint
Features and Type
The knee joint is the largest and most complex joint in the human body, essential for weight-bearing and movement. It is classified as a condylar synovial joint, incorporating two condylar joints between the femur and tibia, and a saddle joint between the femur and patella. The joint cavity is divided by the menisci, making it a complex joint.
Condylar synovial joint: Allows flexion, extension, and limited rotation.
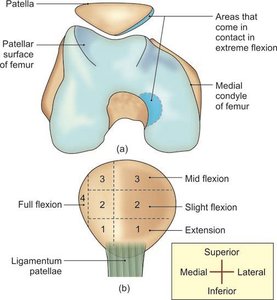
Articular surfaces: Formed by the condyles of the femur, the patella, and the condyles of the tibia.
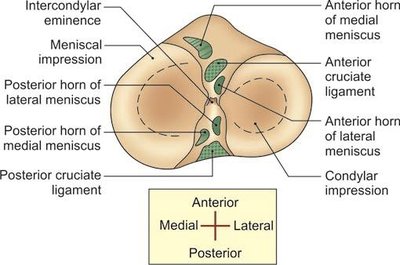
Menisci: Fibrocartilaginous structures that divide the joint cavity and aid in shock absorption.
Ligaments of the Knee Joint
The stability of the knee joint is maintained by several ligaments, which prevent excessive movement and injury.
Fibrous capsule: Encloses the joint.
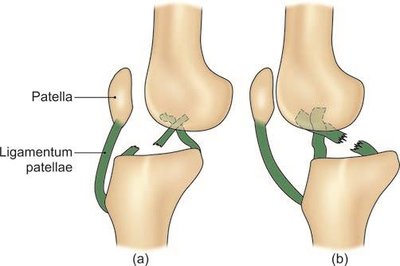
Ligamentum patellae: Connects the patella to the tibia.
Tibial (medial) collateral ligament: Provides medial stability.
Fibular (lateral) collateral ligament: Provides lateral stability.
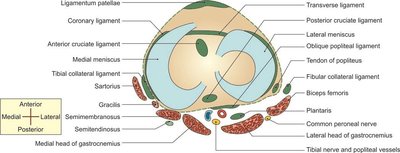
Oblique and arcuate popliteal ligaments: Reinforce the posterior aspect.
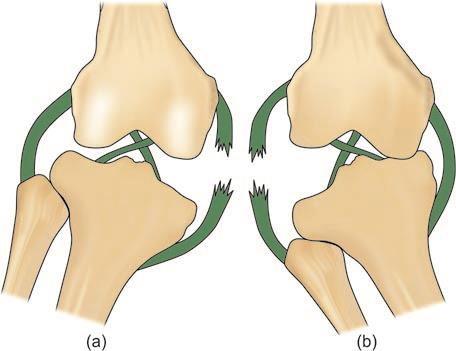
Anterior and posterior cruciate ligaments: Prevent anterior and posterior displacement of the tibia.
Medial and lateral meniscus: Shock absorption and joint congruency.
Transverse ligament: Connects the menisci.
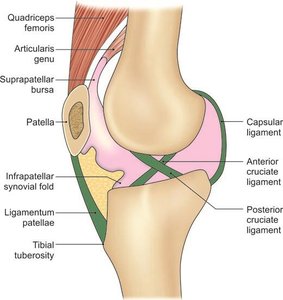
Synovial Membrane and Bursae
The synovial membrane lines the capsule of the knee joint, except posteriorly where it is reflected by the cruciate ligaments. It forms a common covering for both ligaments. Numerous bursae surround the knee, reducing friction between tendons, ligaments, and bone.
Anterior bursae: Subcutaneous prepatellar, subcutaneous infrapatellar, deep infrapatellar, suprapatellar.
Lateral bursae: Located near the lateral head of gastrocnemius, fibular collateral ligament, biceps femoris, popliteus tendon.
Medial bursae: Near the medial head of gastrocnemius, anserine bursa, tibial collateral ligament, semimembranosus.
Relations of the Knee Joint
The knee joint is surrounded by various muscles, tendons, nerves, and vessels, which are important for its function and clinical assessment.
Anterior: Quadriceps femoris, patella, ligamentum patellae.
Posterior: Popliteal vessels, tibial nerve, heads of gastrocnemius.
Medial: Sartorius, gracilis, semimembranosus, tibial collateral ligament.
Blood Supply
The knee joint receives blood from multiple arteries, ensuring adequate nutrition and healing capacity.
Five genicular branches of the popliteal artery
Descending genicular branch of the femoral artery
Descending branch of the lateral circumflex femoral artery
Two recurrent branches of the anterior tibial artery
Circumflex fibular branch of the posterior tibial artery
Nerve Supply
The knee joint is innervated by branches of the femoral, tibial, and common peroneal nerves, which are important for movement and pain sensation.
Femoral nerve
Tibial nerve (branch of sciatic)
Common peroneal nerve (branch of sciatic)
Movements at the Knee Joint
The knee joint allows several movements, primarily flexion and extension, as well as limited medial and lateral rotation. These movements are essential for walking, running, and standing.
Flexion: Bending the knee, decreasing the angle between femur and tibia.
Extension: Straightening the knee, increasing the angle.
Medial rotation: Rotating the tibia inward (occurs in flexed position).
Lateral rotation: Rotating the tibia outward (occurs in flexed position).
Locking and unlocking: Locking allows the knee to remain extended with minimal muscular effort, primarily through medial rotation of the femur. Unlocking is achieved by the popliteus muscle, which laterally rotates the femur.
Clinical Anatomy
Understanding the clinical aspects of the knee joint is crucial for diagnosing and managing injuries and diseases.
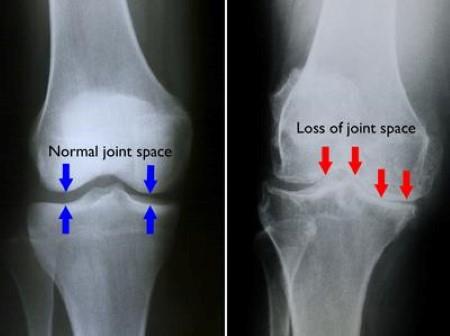
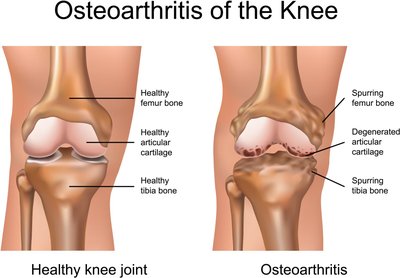
Osteoarthritis: Degenerative joint disease characterized by loss of cartilage and joint space.
Injuries: Meniscal tears, cruciate ligament ruptures, collateral ligament injuries.
Joint replacement: May be necessary if the hip or knee joint is beyond repair.
Muscle atrophy: Vastus medialis is the first to atrophy and last to recover in knee joint disease.
Facts to Remember
The knee joint is the most complicated joint in the body.
Flexion and extension occur in the upper compartment; rotation occurs in the lower (meniscotibial) compartment.
Locking muscle: Vastus medialis (part of quadriceps femoris).
Unlocking muscle: Popliteus.
Fibula does not participate in the knee joint but is involved in the ankle joint.
Talus has no muscular attachment; tendon of flexor hallucis longus passes between its tubercles.
The big toe bears double the weight compared to other toes.
Additional info:
The knee joint is a frequent site of injury due to its complex structure and weight-bearing function.
Proper understanding of the anatomy and biomechanics is essential for clinical assessment and treatment.
