 Back
BackThe Renal System: Regulation, Reabsorption, and Urine Formation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Renal System: Regulation, Reabsorption, and Urine Formation
Regulation of Glomerular Filtration Rate (GFR)
The glomerular filtration rate (GFR) is tightly regulated to ensure proper filtration of blood and maintenance of homeostasis. Both intrinsic and extrinsic mechanisms are involved in this regulation.
Extrinsic Mechanisms: These override intrinsic renal autoregulation during times of extreme stress, prioritizing blood flow to vital organs.
Neural Controls: The sympathetic nervous system (SNS) induces vasoconstriction of afferent arterioles, reducing GFR to conserve blood volume for the heart, brain, and skeletal muscles.
Renin-Angiotensin Mechanism: This hormonal system is activated by direct SNS stimulation, reduced filtrate osmolarity, or decreased stretch of granular cells. Renin converts angiotensinogen to angiotensin I, which is then converted to angiotensin II by angiotensin-converting enzyme (ACE). Angiotensin II is a potent vasoconstrictor and stimulates aldosterone release, increasing sodium and water reabsorption, ultimately raising blood pressure and extracellular fluid (ECF) volume.
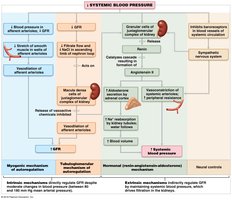
Key Point: The renin-angiotensin system's main purpose is to stabilize systemic blood pressure and ECF volume, not just regulate renal function.
Tubular Reabsorption: Principles and Mechanisms
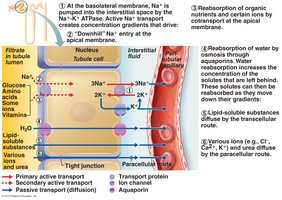
Most of the filtrate produced by the kidneys is reabsorbed, preventing excessive loss of water and essential solutes. Reabsorption occurs via active and passive mechanisms, primarily through the cells lining the renal tubules.
Active Tubular Reabsorption: Substances are moved against their electrochemical gradients, requiring ATP. Sodium reabsorption is the primary active process, creating gradients for the reabsorption of glucose, amino acids, and other ions via secondary active transport.
Passive Tubular Reabsorption: Involves diffusion, facilitated diffusion, and osmosis along electrochemical gradients. Water reabsorption follows sodium via aquaporins (obligatory water reabsorption), and lipid-soluble substances can diffuse passively.
Transport Maximum (Tm): Each transport system has a maximum rate; when exceeded, excess solute appears in urine (e.g., glucose in diabetes mellitus).
Routes of Tubular Reabsorption
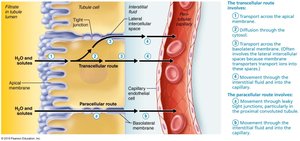
Reabsorption can occur via two main routes:
Transcellular Route: Substances pass through the tubule cell, similar to intestinal absorption.
Paracellular Route: Substances move between tubule cells, mainly water and some ions, especially in the proximal convoluted tubule (PCT) where tight junctions are leaky.
Substances Not Reabsorbed by the Kidney
Certain substances are poorly reabsorbed due to lack of carriers, low lipid solubility, or large size. These include:
Urea: Main nitrogenous waste; about 50-60% is reabsorbed.
Creatinine: Large, lipid-insoluble; not reabsorbed, making it useful for measuring GFR.
Uric Acid: End product of purine metabolism; some is reabsorbed, but excess can lead to gout.
Regional Differences in Tubular Reabsorption
Different segments of the nephron have specialized roles in reabsorption:
Proximal Convoluted Tubule (PCT): Reabsorbs all glucose and amino acids, 65% of Na+ and water, 90% of bicarbonate, and 50% of Cl- and K+.
Loop of Henle (Nephron Loop): Descending limb is permeable to water but not NaCl; ascending limb is permeable to NaCl but not water.
Distal Convoluted Tubule (DCT) and Collecting Duct: Final adjustments in NaCl and water reabsorption are hormonally regulated (ADH, aldosterone, ANP).

Tubular Secretion
Tubular secretion is the process by which substances are added to the filtrate from the blood, primarily in the PCT, late DCT, and early collecting ducts. This process is essential for:
Disposing of substances not filtered initially (e.g., drugs bound to plasma proteins)
Eliminating substances that were passively reabsorbed (e.g., urea, uric acid)
Removing excess K+ ions
Regulating blood pH by secreting H+
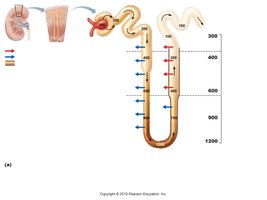
Countercurrent Mechanism and Medullary Osmotic Gradient
The countercurrent mechanism in the nephron loop (loop of Henle) establishes and maintains a medullary osmotic gradient, allowing the kidneys to concentrate or dilute urine as needed.
Descending Limb: Permeable to water but not solutes; water exits by osmosis, increasing filtrate osmolality.
Ascending Limb: Impermeable to water; actively transports NaCl out, decreasing filtrate osmolality.
Countercurrent Multiplier: The interaction between the two limbs amplifies the gradient, essential for water reabsorption in the collecting duct.
Role of Antidiuretic Hormone (ADH) in Urine Concentration
ADH regulates the permeability of the collecting ducts to water, thus controlling urine concentration and volume.
Formation of Dilute Urine: In the absence of ADH, collecting ducts are impermeable to water, resulting in dilute urine (as low as 100 mOsm).
Formation of Concentrated Urine: ADH increases water channel (aquaporin) insertion in collecting duct cells, allowing water reabsorption and production of concentrated urine. This process is vital during dehydration or high plasma osmolarity.


Diuretics: Definition and Examples
A diuretic is any substance that increases urinary output by either not being reabsorbed or by exceeding the renal reabsorption capacity. Common examples include caffeine and certain drugs that inhibit Na+ reabsorption, leading to increased water loss.
Alcohol: Inhibits ADH release, increasing urine output.
Caffeine: Inhibits Na+ reabsorption, increasing urine volume.

Renal Clearance
Renal clearance is the volume of plasma from which a substance is completely cleared by the kidneys per unit time. It is calculated as:
U: Concentration of substance in urine (mg/ml)
V: Urine flow rate (ml/min)
P: Concentration of substance in plasma (mg/ml)
Interpretation:
If RC (substance) = RC (inulin): Substance is filtered but neither reabsorbed nor secreted (e.g., inulin, GFR standard).
If RC (substance) < RC (inulin): Substance is reabsorbed (e.g., urea).
If RC (substance) > RC (inulin): Substance is secreted (e.g., creatinine, drug metabolites).
If RC (substance) = 0: Substance is completely reabsorbed or not filtered (e.g., glucose under normal conditions).
Physical and Chemical Characteristics of Urine
Normal urine is clear to pale yellow due to urochrome pigment. Its odor, pH, and chemical composition can vary based on diet, hydration, and health status.
Color: Deep yellow indicates concentrated urine; cloudiness may indicate infection.
Odor: Ammonia odor develops if urine stands; certain foods and diseases can alter odor.
pH: Normally around 6, but ranges from 4.5 to 8 depending on diet.
Chemical Composition: 95% water, 5% solutes (urea, Na+, K+, phosphate, sulfate, creatinine, uric acid).
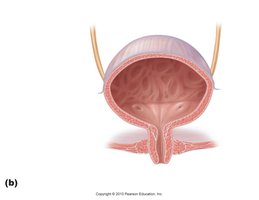
Regulation of Micturition (Urination)
Micturition is the process of emptying the bladder. It involves both involuntary and voluntary neural controls.
Steps:
Detrusor muscle contracts
Internal urethral sphincter opens
External urethral sphincter opens (voluntary control)
Stretch receptors in the bladder wall trigger a reflex arc, sending signals to the spinal cord and brain, resulting in the urge to void.
Voluntary relaxation of the external sphincter allows urination; the reflex subsides if urination is delayed.

Disorders of Micturition
Incontinence: Inability to control urination voluntarily, often due to weakened pelvic floor muscles, pregnancy, or nervous system disorders.
Stress Incontinence: Leakage of urine during activities that increase abdominal pressure (e.g., coughing, sneezing).
Urinary Retention: Inability to expel urine, which may occur after anesthesia or due to prostate enlargement.
