 Back
BackThe Respiratory System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System
Overview and Subdivisions
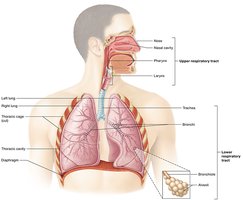
The respiratory system is responsible for the exchange of gases (oxygen and carbon dioxide) between the body and the environment. It is structurally and functionally divided into distinct regions to facilitate this process.
Structural Divisions:
Upper respiratory system: Includes the nose to the pharynx; some parts are shared with the digestive system.
Lower respiratory system: Extends from the glottis to the lungs; dedicated solely to respiration.
Functional Divisions:
Conducting zone: All structures except the lungs; also called "dead space" as no gas exchange occurs here.
Respiratory zone: The lungs, where actual gas exchange takes place.
Structures of the Respiratory System
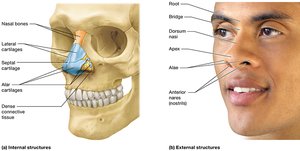
The Nose
The nose is the primary entryway for air into the respiratory system and plays a crucial role in filtering, warming, humidifying, and detecting odors in inhaled air.
External nose: Visible part projecting from the face.
Nares (nostrils): Openings to the nasal cavity.
Internal nose: Located behind the nasal vestibule, divided by the septum and further subdivided by the nasal conchae into passages called nasal meatuses.
Olfactory receptors: Located in the olfactory epithelium, responsible for the sense of smell.
Connections: Linked to sinus cavities and nasolacrimal ducts.
Functions: Smell, air conditioning (warming/cooling), humidification, and filtration of debris.
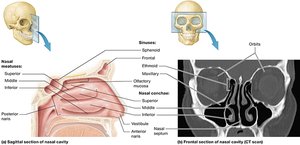
Inner Parts of the Nasal Cavity
The nasal cavity is lined with mucosa and contains structures that increase surface area and turbulence, enhancing air filtration and conditioning.
Nasal conchae: Bony projections that create passages (meatuses) for airflow.
Sinuses: Air-filled spaces that lighten the skull and contribute to voice resonance.
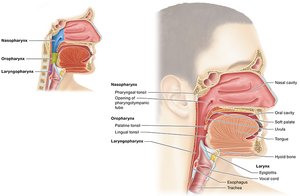
The Pharynx
The pharynx is a muscular tube that serves as a passageway for air, food, and water, and plays a role in speech resonance and immune defense.
Regions:
Nasopharynx: Superior region, behind the nasal cavity.
Oropharynx: Middle region, behind the oral cavity.
Laryngopharynx: Inferior region, contains the epiglottis which directs food and air appropriately.
Lymphatic tissue: Contains lymph nodes to help defend against pathogens.
Functions: Swallowing (deglutition), passageway for food/air/water, and speech resonance.
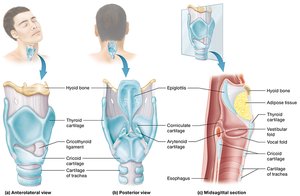
The Larynx
The larynx (voice box) connects the pharynx to the trachea and is essential for sound production, airway protection, and passage of air.
Epiglottis: Covers the glottis during swallowing to prevent food from entering the lower respiratory tract.
Cartilage structures: Nine cartilages, including the thyroid cartilage (Adam’s apple).
Ventricular folds (false vocal cords): Superior, help seal the larynx during breath holding.
Vocal folds (true vocal cords): Inferior, vibrate to produce sound.
Cilia and mucus: Trap debris and move it upward toward the pharynx.
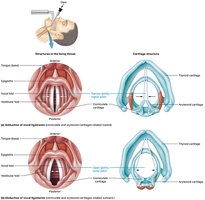
Speech Production
Speech is produced as air passes over the vocal folds, causing them to vibrate. The pitch and volume are modified by the tension and length of the folds, which are influenced by muscles and hormones (e.g., androgens). The pharynx amplifies the sound, and the tongue and mouth further modify it before it exits the body.
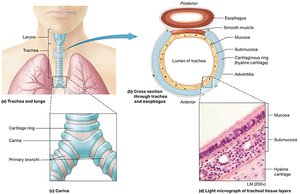
The Trachea
The trachea (windpipe) is a tube that conducts air from the larynx to the bronchi. It is supported by C-shaped rings of hyaline cartilage that keep the airway open.
Layers:
Mucosa: Lined with cilia and mucus to trap particles.
Submucosa: Contains glands and connective tissue.
Hyaline cartilage: Provides structural support.
Adventitia: Outermost connective tissue layer.
Carina: The point where the trachea splits into the primary bronchi; sensitive and triggers coughing.
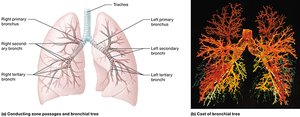
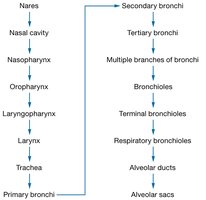
The Bronchi and Bronchial Tree
The bronchi are airways that branch from the trachea into the lungs, forming a highly branched bronchial tree that conducts air to the alveoli.
Primary bronchi: Enter each lung.
Secondary (lobar) bronchi: Supply each lobe of the lungs.
Tertiary bronchi, bronchioles, terminal bronchioles: Successive branches with decreasing cartilage and increasing smooth muscle.
Autonomic control: Sympathetic stimulation dilates bronchi; parasympathetic constricts them.
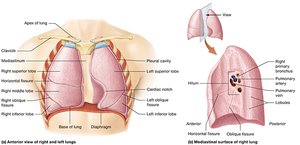
The Lungs
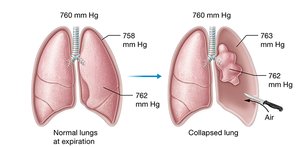
The lungs are paired organs where gas exchange occurs. The left lung is smaller due to the cardiac notch, and each lung is divided into lobes and surrounded by pleural membranes.
Left lung: Two lobes, one fissure, cardiac notch.
Right lung: Three lobes, two fissures.
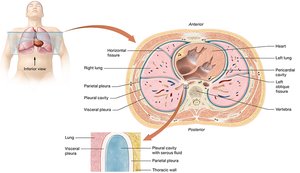
Pleural membranes:
Visceral pleura: Covers the lungs.
Parietal pleura: Lines the thoracic cavity.
Pleural cavity: Space between membranes, filled with fluid to reduce friction.
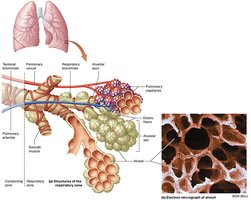
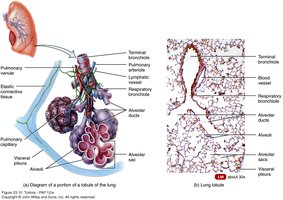
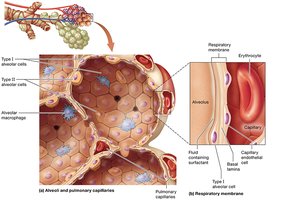
Alveoli and Gas Exchange
Alveoli are tiny, grape-like sacs at the end of the respiratory tree where gas exchange occurs. Each alveolar sac contains multiple alveoli, and the walls are extremely thin to facilitate rapid diffusion of gases.
Type I alveolar cells: Form the majority of the alveolar wall; site of gas exchange.
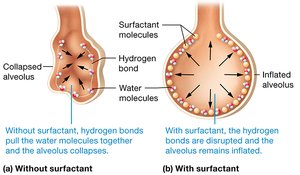
Type II alveolar cells: Secrete surfactant to reduce surface tension and prevent alveolar collapse.
Respiratory membrane: Composed of alveolar epithelium, basement membranes, and capillary endothelium; approximately 0.5 µm thick.
Summary Table: Respiratory System Structures and Functions
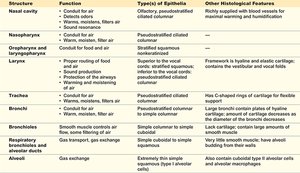
Structure | Function | Epithelium Type | Other Features |
|---|---|---|---|
Nasal cavity | Conducts, filters, warms, humidifies air | Olfactory, pseudostratified ciliated columnar | Rich blood supply, mucus for humidification |
Nasopharynx | Conducts air | Pseudostratified ciliated columnar | Contains tonsils |
Oropharynx/Laryngopharynx | Food and air passage, speech resonance | Stratified squamous | Framework of cartilage |
Larynx | Sound production, air passage | Pseudostratified ciliated columnar | Contains vocal cords |
Trachea | Conducts air | Pseudostratified ciliated columnar | C-shaped cartilage rings |
Bronchi | Conducts air | Pseudostratified to simple columnar | Cartilage plates, smooth muscle |
Bronchioles | Air transport, some gas exchange | Simple columnar to simple cuboidal | Lack cartilage, more smooth muscle |
Alveoli | Gas exchange | Simple squamous (Type I) | Surfactant, macrophages |
Mechanics of Breathing
Parts of Respiration
Pulmonary ventilation: Movement of air into and out of the lungs (inhalation and exhalation).
External respiration: Exchange of gases between alveoli and blood.
Internal respiration: Exchange of gases between blood and body tissues.
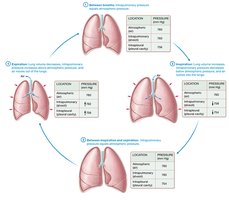
Boyle’s Law and Pressure Changes
Boyle’s Law states that the pressure of a gas is inversely proportional to its volume, assuming constant temperature and amount of gas:
As lung volume increases, pressure decreases, causing air to flow in; as volume decreases, pressure increases, causing air to flow out.
Inhalation and Exhalation
Inhalation: Active process; diaphragm contracts and flattens, intercostal muscles expand the rib cage, increasing thoracic volume and decreasing pressure (to ~758 mmHg), drawing air in.
Exhalation: Passive process; diaphragm relaxes, thoracic volume decreases, pressure increases (to ~762 mmHg), pushing air out.
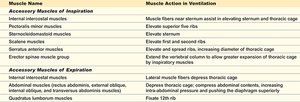
Muscles Involved in Breathing
Muscle Name | Action in Ventilation |
|---|---|
Diaphragm | Primary muscle of inspiration; flattens to increase thoracic volume |
External intercostals | Elevate ribs, expanding thoracic cavity |
Accessory muscles | Assist in deep or forced breathing |
Internal intercostals, abdominal muscles | Active during forced expiration |
Airflow, Surface Tension, and Surfactant
Surface tension: Caused by hydrogen bonds in water lining the alveoli; tends to collapse alveoli.
Surfactant: Secreted by Type II alveolar cells; reduces surface tension, preventing alveolar collapse.
Lung compliance: Measure of lung stretchability; high compliance means easier expansion.
Airway resistance: Friction in airways; smaller diameter increases resistance and decreases airflow.
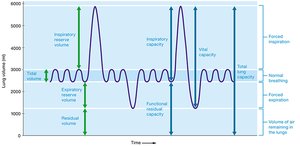
Lung Volumes and Capacities
Lung volumes and capacities are measured to assess respiratory health and function.
Tidal volume (TV): Air moved in and out during normal breathing.
Inspiratory reserve volume (IRV): Extra air inhaled after a normal inspiration.
Expiratory reserve volume (ERV): Extra air exhaled after a normal expiration.
Residual volume (RV): Air remaining in lungs after maximal exhalation.
Vital capacity (VC): Maximum air exhaled after maximal inhalation.
Gas Laws and Gas Exchange
Dalton’s Law of Partial Pressures
Each gas in a mixture exerts its own pressure, called partial pressure. The total pressure is the sum of all partial pressures:
Gases diffuse from areas of higher to lower partial pressure; the greater the gradient, the faster the diffusion.
Henry’s Law
The amount of gas that dissolves in a liquid is proportional to its partial pressure and solubility. CO2 is more soluble in blood than O2 or N2.
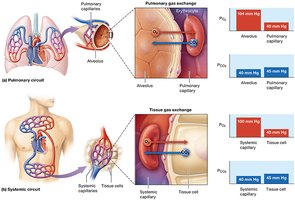
External and Internal Respiration
External respiration: O2 diffuses from alveoli (105 mmHg) to blood (40 mmHg); CO2 diffuses from blood (45 mmHg) to alveoli (40 mmHg).
Internal respiration: O2 diffuses from blood (100 mmHg) to tissues (40 mmHg); CO2 diffuses from tissues (45 mmHg) to blood (40 mmHg).
Factors Affecting Gas Exchange Rate
Molecular weight: Larger molecules diffuse more slowly.
Diffusion distance: Thicker membranes slow diffusion.
Surface area: Greater area increases exchange rate.
Solubility: Higher solubility increases diffusion (CO2 diffuses faster than O2).
Partial pressure gradient: Larger gradients increase diffusion rate.
Transport of Gases in the Blood
Oxygen Transport
~1.5% of O2 is dissolved in plasma due to low solubility.
~98.5% is bound to hemoglobin (Hb) in red blood cells, forming oxyhemoglobin.
Each Hb molecule can bind up to 4 O2 molecules.

Factors Affecting Hemoglobin-Oxygen Affinity
Partial pressure of O2: Higher PO2 increases Hb saturation.
pH (Bohr Effect): Increased CO2 lowers pH, decreasing Hb affinity for O2.
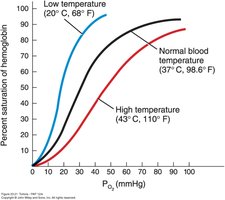
Temperature: Higher temperature decreases Hb affinity for O2.
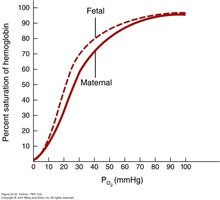
Fetal Hb: Has higher affinity for O2 than adult Hb, facilitating maternal-fetal O2 transfer.

Carbon Dioxide Transport
~7% dissolved in plasma as CO2.
~23% bound to Hb as carbaminohemoglobin.
~70% transported as bicarbonate ions (HCO3-), catalyzed by carbonic anhydrase:

Chloride Shift
To maintain electrical neutrality, chloride ions (Cl-) move into or out of red blood cells as bicarbonate ions are exchanged during CO2 transport.
Control of Respiration
Nervous System Regulation
Breathing is regulated by respiratory centers in the brainstem (medulla and pons), which respond to chemical and neural signals to maintain homeostasis.
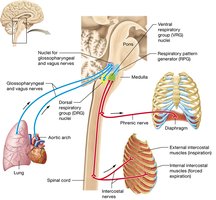
Homeostatic Mechanisms
Respiratory rate is adjusted in response to changes in blood CO2, O2, and pH, as well as voluntary control and stretch receptors in the lungs.

Respiratory Disorders
Restrictive Lung Diseases
Idiopathic pulmonary fibrosis
Pneumoconiosis
Neuromuscular disorders
All prevent normal exhalation
Chronic Obstructive Pulmonary Disease (COPD)
Emphysema
Small airway disease
Chronic bronchitis
Asthma
Lung cancer
