 Back
BackThe Respiratory System: Structure, Function, and Clinical Considerations
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System: Overview and Structural Plan
Introduction to the Respiratory System
The respiratory system is essential for gas exchange, supplying oxygen to the body and removing carbon dioxide. Its structure resembles an inverted tree, with the trachea as the trunk and alveoli as the leaves, where gas exchange occurs via diffusion.
Primary Functions: Air distribution, gas exchange, air purification, and vocalization.
Gas Exchange: Occurs by diffusion across the alveolar and capillary membranes.
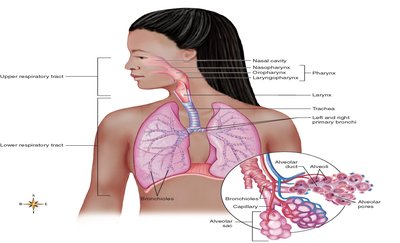
Structural Organization of the Respiratory System
Upper Respiratory Tract: Nose, pharynx, larynx
Lower Respiratory Tract: Trachea, bronchial tree, lungs
Respiratory Mucosa and Air Purification
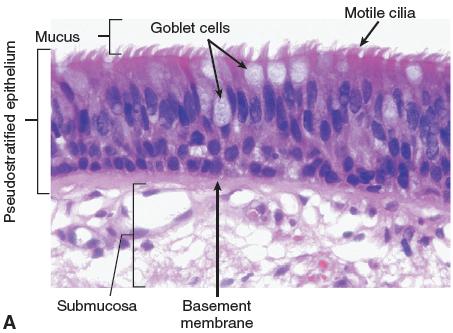
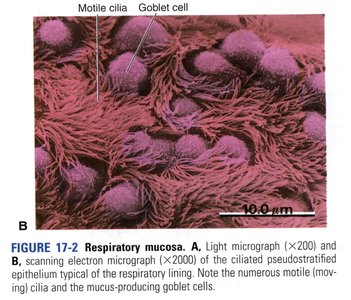
Structure and Function of Respiratory Mucosa
The respiratory mucosa is a mucous membrane lining the airways, producing over 125 mL of mucus daily. This mucus forms a 'mucus blanket' that traps dust, pollen, and other irritants. Cilia on mucosal cells move the mucus upward toward the pharynx for removal, serving as a critical air purification mechanism.
Epithelium: Pseudostratified ciliated columnar epithelium with goblet cells.
Function: Traps and removes particulates, humidifies air, and protects lower airways.
Anatomy of the Upper Respiratory Tract
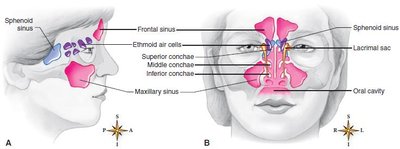
Nose and Paranasal Sinuses
The nose is divided by the nasal septum and lined with mucous membrane. Paranasal sinuses (frontal, maxillary, sphenoidal, ethmoidal) drain into the nasal cavity and help warm, moisten, and filter air. The nose also houses olfactory receptors for the sense of smell.
Pharynx (Throat)
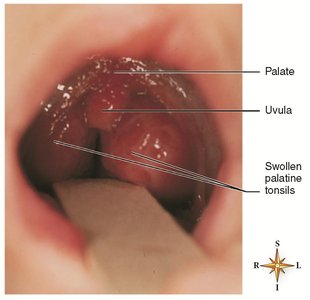
The pharynx is a muscular tube about 12.5 cm long, divided into three regions: nasopharynx, oropharynx, and laryngopharynx. It serves as a passageway for both air and food and contains lymphoid tissue (tonsils) for immune protection.
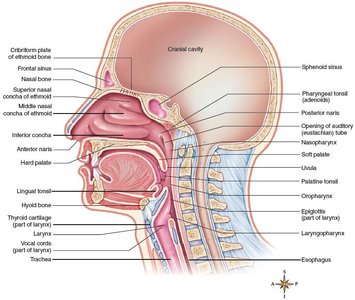
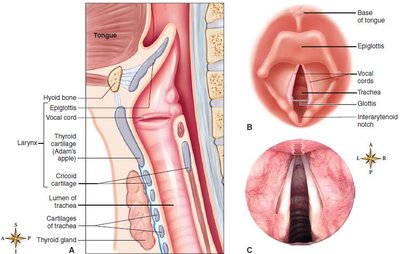
Larynx (Voice Box)
The larynx is located below the pharynx and is composed of several cartilages, including the thyroid cartilage (Adam's apple) and the epiglottis, which prevents food from entering the airway. The larynx contains the vocal cords, which vibrate to produce sound.
Lower Respiratory Tract: Trachea, Bronchi, and Lungs
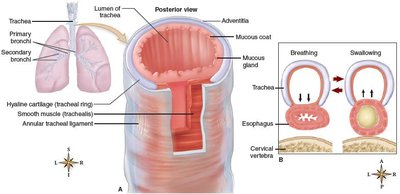
Trachea (Windpipe)
The trachea is a tube about 11 cm long, supported by C-shaped rings of cartilage that keep it open. It conducts air from the larynx to the bronchi and is lined with mucosa for air purification.
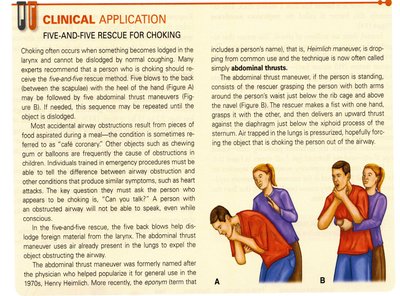
Clinical Considerations: Airway Obstruction and Tracheostomy
Obstruction of the trachea can be life-threatening. The abdominal thrust maneuver (Heimlich maneuver) is used to clear obstructions. In severe cases, a tracheostomy may be performed to bypass the blockage.
Bronchi, Bronchioles, and Alveoli
The trachea divides into right and left primary bronchi, which branch into smaller bronchi and bronchioles, ending in clusters of alveoli. The right bronchus is more vertical, making it more likely for aspirated objects to enter the right lung.
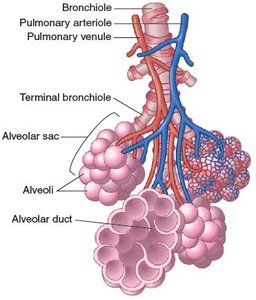
Bronchi/Bronchioles: Distribute air to alveoli.
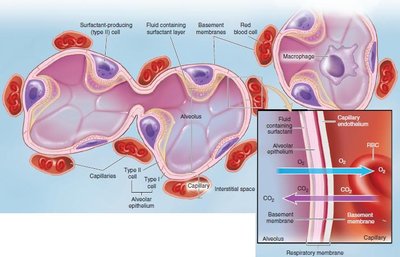
Alveoli: Site of gas exchange; Type II cells produce surfactant to reduce surface tension.
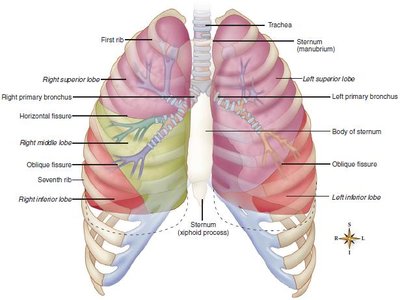
Lungs and Pleura
The lungs are divided into lobes (three on the right, two on the left) and are covered by the pleura, a double-layered membrane that reduces friction during breathing. The apex is the narrow upper part, and the base rests on the diaphragm.
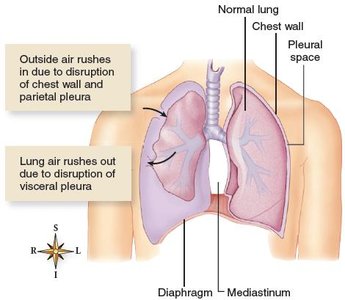
Pleural Disorders
Pleurisy: Inflammation of the pleura, causing pain during breathing.
Atelectasis: Collapse of lung tissue, often due to pneumothorax (air in pleural space) or hemothorax (blood in pleural space).
Respiratory Physiology: Mechanics and Regulation
Mechanics of Breathing (Pulmonary Ventilation)
Breathing consists of inspiration (active process) and expiration (usually passive). Inspiration increases thoracic volume via contraction of the diaphragm and external intercostals, decreasing lung pressure and drawing air in. Expiration occurs as the thorax returns to resting size, increasing pressure and expelling air.
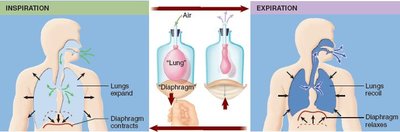
Inspiration: Diaphragm contracts and flattens; external intercostals elevate ribs.
Expiration: Usually passive; forced expiration uses internal intercostals and abdominal muscles.
Volumes of Air Exchanged
Air volumes are measured with a spirometer:
Tidal Volume (TV): Normal breath in or out.
Vital Capacity (VC): Maximum air exhaled after maximum inhalation.
Expiratory Reserve Volume (ERV): Extra air exhaled after normal expiration.
Inspiratory Reserve Volume (IRV): Extra air inhaled after normal inspiration.
Residual Volume (RV): Air remaining after maximal expiration.
Regulation of Respiration
Respiratory control centers in the brainstem (medulla and pons) regulate breathing rate and depth. Chemoreceptors in the carotid and aortic bodies respond to changes in CO2, O2, and pH. Pulmonary stretch receptors prevent overinflation of the lungs.
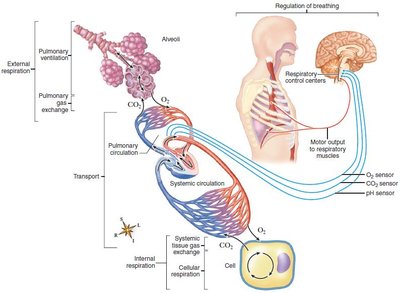
Gas Exchange and Transport
Pulmonary and Systemic Gas Exchange
Oxygen diffuses from alveoli into capillary blood, binding to hemoglobin to form oxyhemoglobin. Carbon dioxide diffuses from blood into alveoli for expiration. In tissues, oxygen is released from hemoglobin, and carbon dioxide is picked up for transport back to the lungs.
Oxygen Transport: Mostly as oxyhemoglobin (HbO2).
Carbon Dioxide Transport: Dissolved (10%), as carbaminohemoglobin (20%), and as bicarbonate ions (70%).
Clinical Conditions and Disorders
Upper and Lower Respiratory Tract Disorders
Upper Respiratory Infections (URIs): Rhinitis, pharyngitis, laryngitis, epiglottitis, croup.
Anatomical Conditions: Deviated septum, epistaxis (nosebleed).
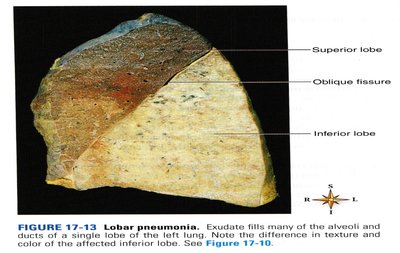
Lower Respiratory Disorders: Acute bronchitis, pneumonia, tuberculosis, restrictive and obstructive pulmonary disorders (COPD, chronic bronchitis, emphysema, asthma), lung cancer.
Summary Table: Key Structures and Functions of the Respiratory System
Structure | Main Function |
|---|---|
Nose/Nasal Cavity | Warms, moistens, filters air; olfaction |
Pharynx | Passageway for air and food; immune defense |
Larynx | Air passage; voice production |
Trachea | Conducts air to bronchi; air purification |
Bronchi/Bronchioles | Air distribution |
Alveoli | Gas exchange |
Pleura | Reduces friction during breathing |
Key Equations
Gas Exchange (Fick's Law):
Where: J = rate of diffusion D = diffusion coefficient A = surface area (P1 - P2) = partial pressure difference T = thickness of membrane
Oxygen Transport:
Carbon Dioxide Transport (Bicarbonate Reaction):
Additional info:
Surfactant is a phospholipid substance produced by Type II alveolar cells that reduces surface tension, preventing alveolar collapse.
Restrictive pulmonary disorders primarily restrict lung expansion (inspiration), while obstructive disorders impede airflow (expiration).
