 Back
BackThe Spinal Cord and Spinal Nerves: Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Spinal Cord: Structure and General Functions
Overview and Major Functions
The spinal cord is a vital component of the central nervous system, serving as the main conduit for information traveling between the brain and the rest of the body. It is responsible for transmitting sensory input, issuing motor commands, and mediating rapid, involuntary responses known as spinal reflexes.
Structural and Functional Link: Connects the brain to peripheral nerves, integrating sensory and motor information.
Spinal Reflexes: Fast, automatic responses to stimuli that do not require brain involvement, ensuring rapid reaction to environmental changes.
Gross Anatomy of the Spinal Cord
Regions and External Features
The spinal cord extends from the medulla oblongata of the brainstem through the vertebral canal, ending at the conus medullaris near the L1 vertebra. It is divided into four main regions: cervical, thoracic, lumbar, and sacral. Two enlargements (cervical and lumbar) accommodate the increased number of neurons serving the limbs.
Conus Medullaris: Tapered end of the spinal cord.
Cauda Equina: Bundle of nerve roots extending below the conus medullaris.
Longitudinal Depressions: Posterior median sulcus and anterior median fissure run along the dorsal and ventral surfaces, respectively.

Spinal Nerves: Structure and Identification
Organization and Classification
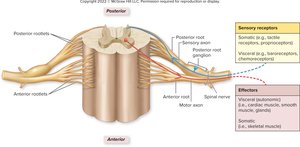
Spinal nerves are mixed nerves containing both sensory and motor fibers. There are 31 pairs, each named according to the region and level of the spinal cord from which they emerge (e.g., C1–C8, T1–T12, L1–L5, S1–S5, Co1).
Connective Tissue Wrappings: Epineurium (outer), perineurium (around fascicles), endoneurium (around individual axons).
Roots and Rootlets: Posterior (dorsal) roots carry sensory fibers; anterior (ventral) roots carry motor fibers. The roots merge to form a mixed spinal nerve.
Protection and Support of the Spinal Cord
Meninges and Spaces
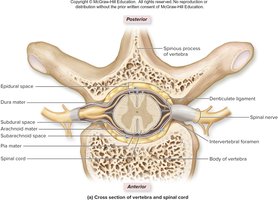
The spinal cord is protected by the vertebral column, three connective tissue membranes (meninges), and cerebrospinal fluid (CSF). The meninges include the pia mater, arachnoid mater, and dura mater, each with distinct structural and functional roles.
Pia Mater: Innermost, delicate layer adhering to the spinal cord; forms denticulate ligaments and filum terminale.
Arachnoid Mater: Middle, web-like layer; subarachnoid space beneath contains CSF.
Dura Mater: Outermost, tough layer; epidural space outside dura contains fat and blood vessels.
Internal Anatomy: Gray and White Matter
Gray Matter Organization
Gray matter in the spinal cord consists of neuron cell bodies, dendrites, and unmyelinated axons. It is organized into horns:
Posterior Horns: Contain sensory interneurons.
Anterior Horns: Contain somatic motor neuron cell bodies.
Lateral Horns: Present in T1–L2; contain autonomic motor neuron cell bodies.
Gray Commissure: Connects left and right sides, surrounds the central canal.

White Matter Organization
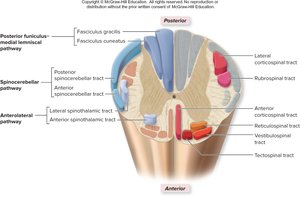
White matter consists of myelinated axons organized into funiculi (columns): posterior, lateral, and anterior. Each funiculus contains ascending (sensory) and descending (motor) tracts, which are further divided into fasciculi.
Posterior Funiculus: Sensory tracts (e.g., fasciculus gracilis, fasciculus cuneatus).
Lateral and Anterior Funiculi: Both sensory and motor tracts.
White Commissure: Connects left and right anterior funiculi.

Spinal Cord Pathways
Sensory Pathways
Sensory (ascending) pathways transmit information from receptors to the brain. They are typically composed of three neurons: primary, secondary, and tertiary.
Posterior Funiculus–Medial Lemniscal Pathway: Carries discriminative touch and proprioceptive information.
Anterolateral Pathway: Transmits pain, temperature, crude touch, and pressure.
Spinocerebellar Pathway: Conveys proprioceptive information to the cerebellum (two-neuron chain).



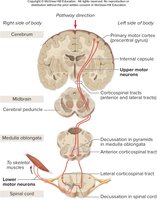
Motor Pathways
Motor (descending) pathways control effectors such as skeletal muscles. They typically involve an upper motor neuron (originating in the brain) and a lower motor neuron (in the spinal cord or brainstem).
Direct (Pyramidal) Pathway: Includes lateral and anterior corticospinal tracts for voluntary movement.
Indirect Pathways: Include rubrospinal, reticulospinal, tectospinal, and vestibulospinal tracts for involuntary control of posture, balance, and reflexive movements.
Spinal Nerve Branches and Distribution
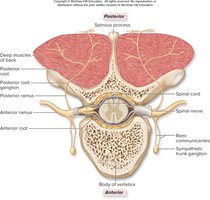
Rami and Plexuses
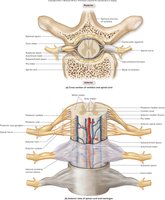
After exiting the vertebral column, each spinal nerve splits into branches (rami):
Posterior Ramus: Innervates muscles and skin of the back.
Anterior Ramus: Innervates anterior and lateral trunk, limbs; forms nerve plexuses.
Rami Communicantes: Connect spinal nerves to the sympathetic trunk ganglia.
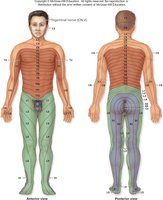
Dermatomes
A dermatome is an area of skin supplied by a single spinal nerve. Dermatomes are clinically important for diagnosing nerve or spinal cord injuries and for understanding referred pain patterns.
Example: T10 dermatome encircles the umbilicus; loss of sensation in a specific dermatome can indicate nerve damage at a particular spinal level.
Nerve Plexuses
Nerve plexuses are networks of interweaving anterior rami. The four main plexuses are cervical, brachial, lumbar, and sacral, each supplying specific regions of the body.
Cervical Plexus (C1–C4): Innervates neck muscles, skin, and diaphragm (via phrenic nerve).
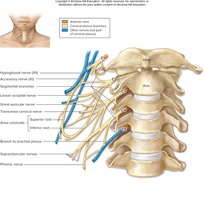
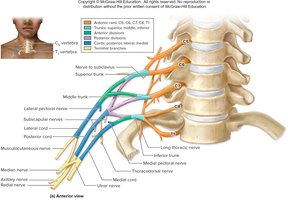
Brachial Plexus (C5–T1): Supplies upper limb; major branches include axillary, median, musculocutaneous, radial, and ulnar nerves.

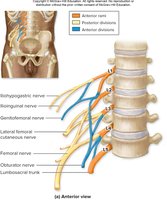
Lumbar Plexus (L1–L4): Innervates anterior and medial thigh, abdominal wall, and portions of external genitalia.

Sacral Plexus (L4–S4): Supplies posterior thigh, most of the lower leg and foot; includes the sciatic nerve (largest in the body).


Reflexes and Reflex Arcs
Characteristics and Components
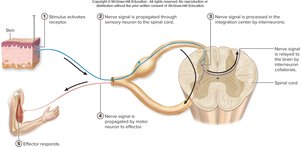
Reflexes are rapid, involuntary, and preprogrammed responses to specific stimuli, serving as protective mechanisms. The neural pathway underlying a reflex is called a reflex arc.
Components of a Reflex Arc: Receptor, sensory neuron, integration center (interneurons), motor neuron, effector.
Classification of Reflexes
By Integration Center: Spinal or cranial
By Effector: Somatic (skeletal muscle) or visceral (smooth/cardiac muscle, glands)
By Number of Synapses: Monosynaptic or polysynaptic
By Laterality: Ipsilateral or contralateral
By Origin: Innate or acquired

Common Spinal Reflexes
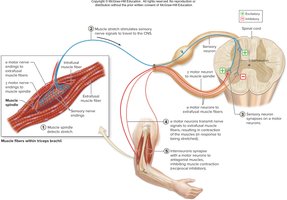
Stretch Reflex: Muscle contraction in response to stretching within the muscle; helps maintain posture and muscle tone.
Tendon (Golgi Tendon) Reflex: Prevents excessive muscle contraction by causing muscle relaxation in response to increased tension.
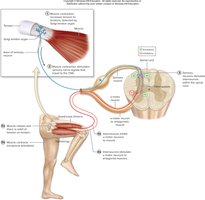
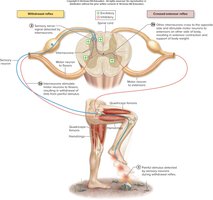
Withdrawal (Flexor) Reflex: Rapid withdrawal of a limb from a painful stimulus.
Crossed-Extensor Reflex: Complements the withdrawal reflex by extending the opposite limb to support body weight.
Clinical Relevance of Reflex Testing
Reflex testing is a valuable diagnostic tool for assessing the integrity of the nervous system. Abnormal reflexes may indicate damage to specific nerves, spinal segments, or regions of the brain.
Hypoactive Reflex: Diminished or absent response; may indicate peripheral nerve or muscle disease.
Hyperactive Reflex: Exaggerated response; may indicate central nervous system damage.
